1. What is stress induced cardiomyopathy?
Stress induced cardiomyopathy (Takotsubo cardiomyopathy) is transient systolic dysfunction involving the apical and/or mid-segments of the left ventricle (LV) with the clinical presentation and laboratory findings of acute myocardial infarction (MI) in the absence of significant coronary artery disease.
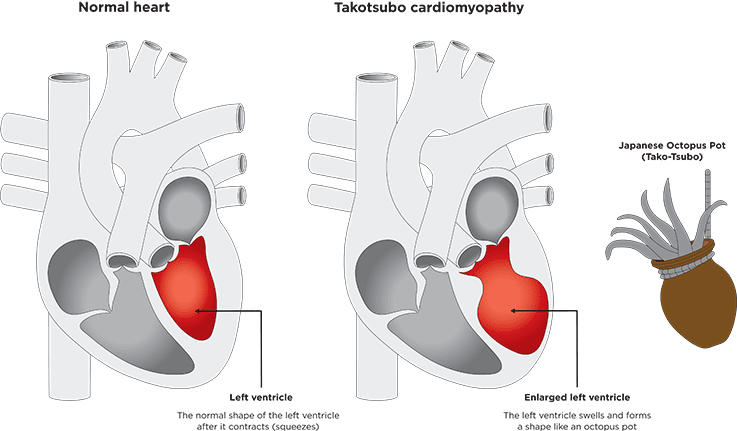
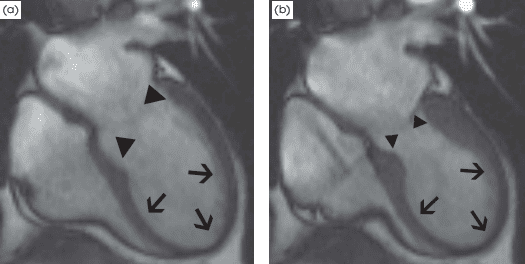
It typically manifests as a cardiomyopathy with depressed contractility of the mid- and apical segments of the LV and increased contractility of the basal walls, producing a characteristic “balloon” appearance.
The syndrome has been aptly named for a Japanese pot for octopus fishing, or “tako-tsubo,” which has a round bottom and narrow neck, which resembles the morphology of the LV in this condition.
Less commonly, it can exclusively affect the mid-ventricle with sparing of the apical LV, or involve both the right and left ventricles.
It is also referred to as broken heart syndrome and apical ballooning syndrome.
2. MRI findings
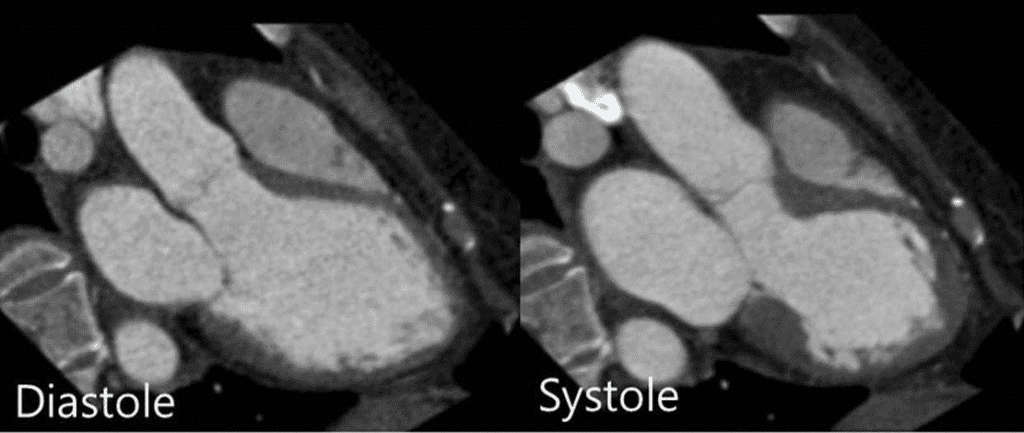
– LV akinesia/hypokinesia in apico-to mid portion and apical ballooning
– Hyperkinesia of basal wall
– High T2 intensity signal (edema) : matches the wall-motion abnormalities seen on cine MRI
– No DCE
– Absence of significant luminal narrowing in epicardial artery
– Normal MRI perfusion
3. Summary
– Transient LV apical ballooning SD
– Acute substernal pain
– Cause : multivessel coronary vasospasm, abnormal coronary microvascular function, catecholamine related cardiotoxicity
– Female older than 50 (80%), emotional/physical stress (65%), good prognosis
Reference)
Charles S. White, Linda B. Haramati, Joseph Jen-Sho Chen, and Jeffrey M. Levsky (2014), Cardiac Imaging, Oxford university press