CARTO
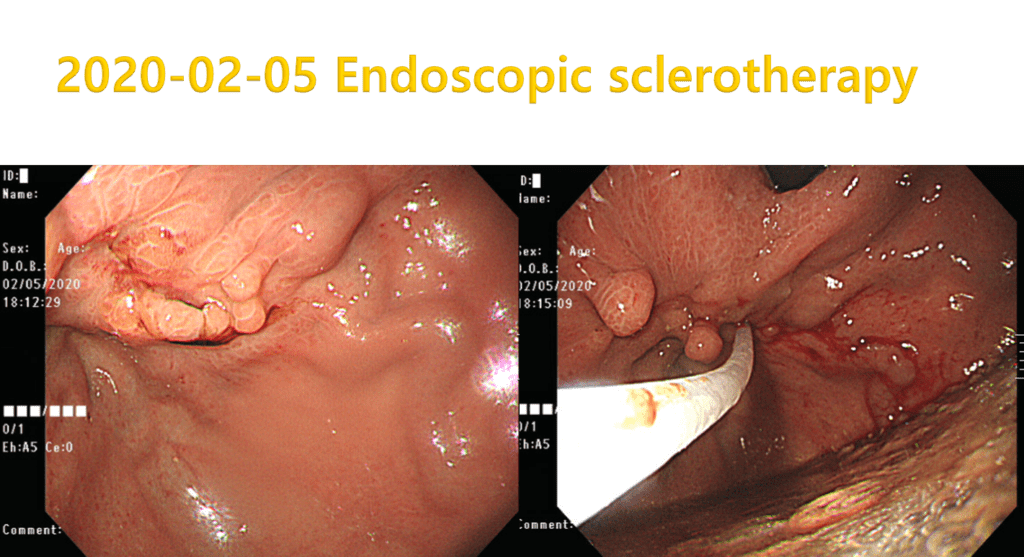
A 50 year-old female patient presented E.R with hematemesis.
Urgent endoscopy was done. See below.
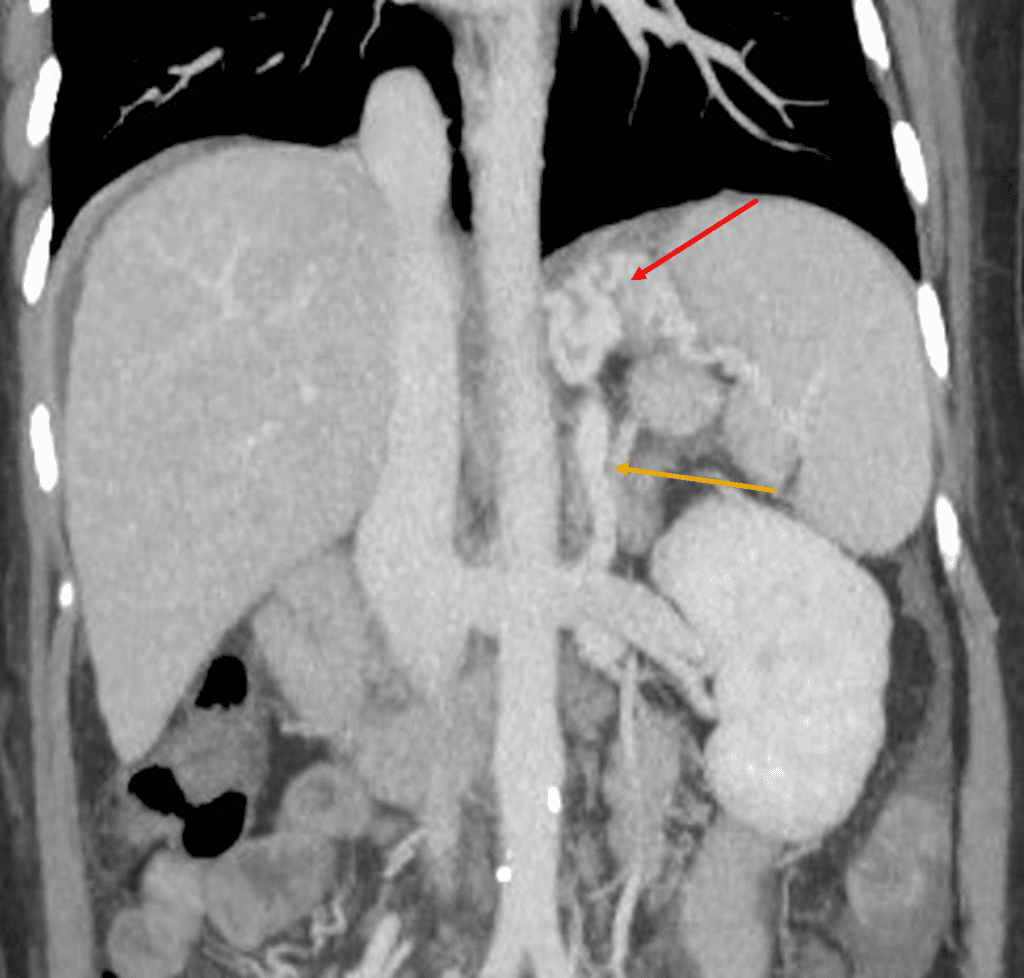
Unfortunately the the patient’s Hemoglobin was not recovered to normal range until 3 days after the procedure and had recurrent melena.
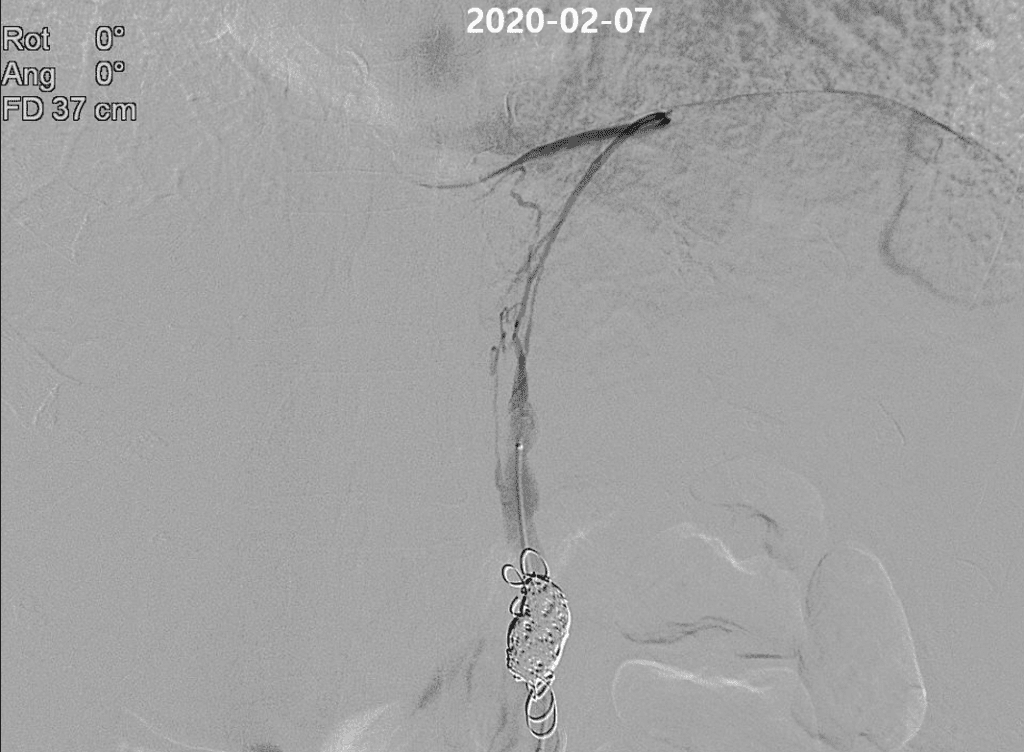
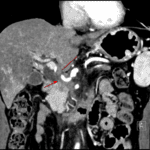
So we planned interventional procedure by reviewing previous CT scan.

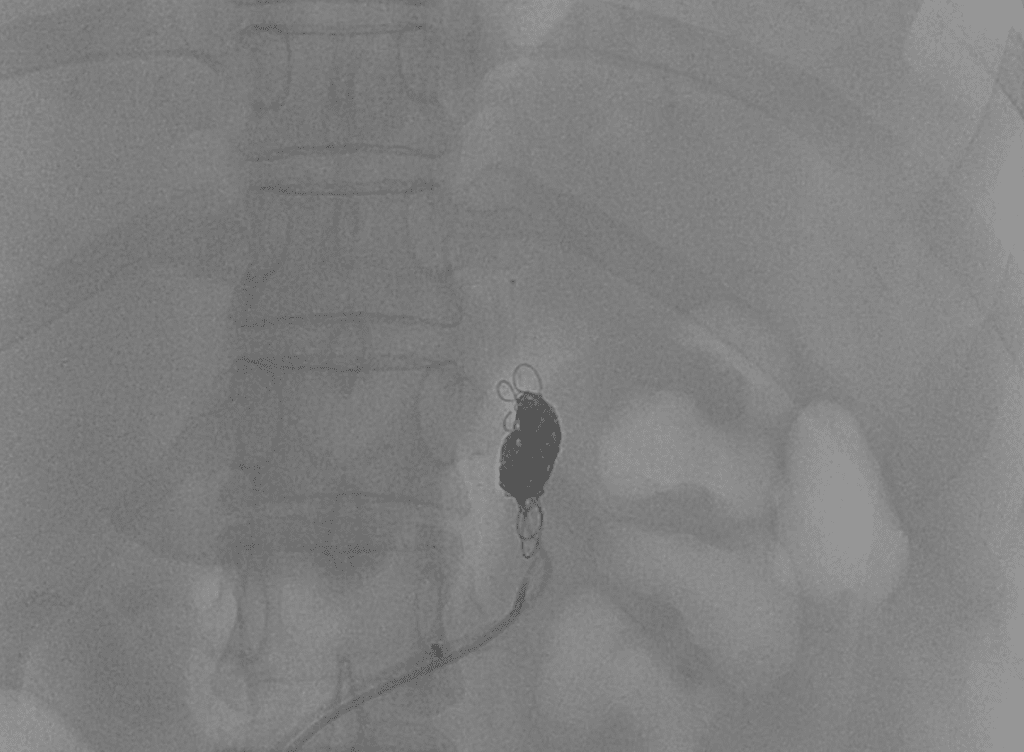


The hemoglobin normalized just one day after the procedure, and there were no signs of bleeding. Consequently, the patient was discharged three days after the procedure. Two weeks later, the patient returned to the clinic in good condition.
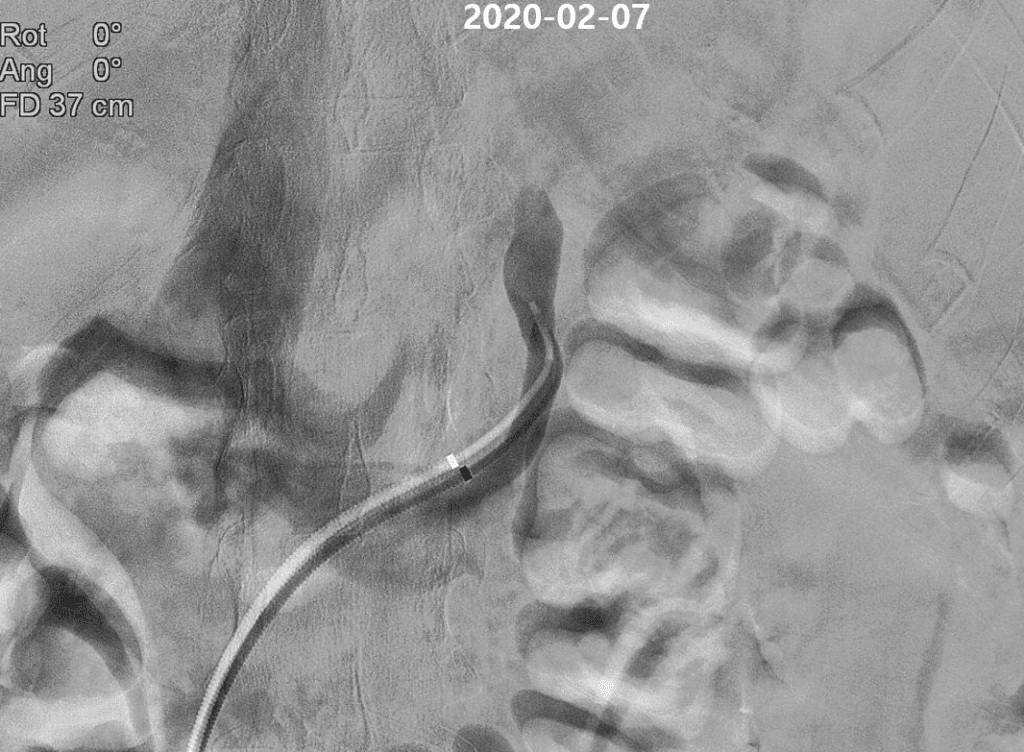
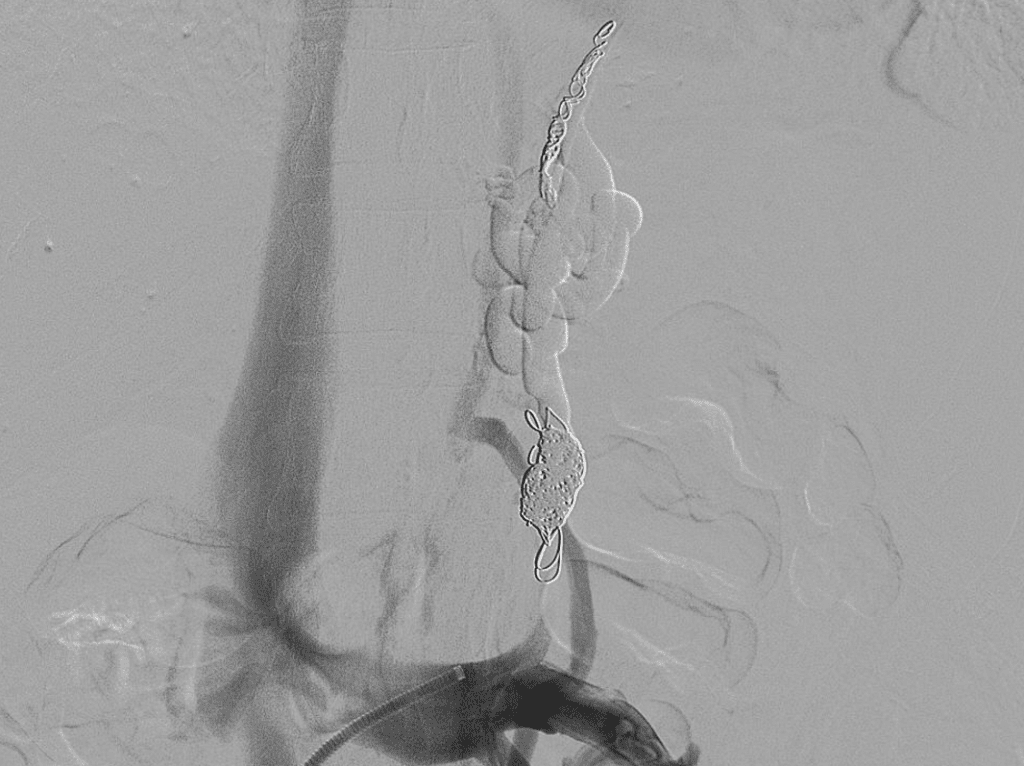
What we performed is called ‘Coil Assisted Retrograde Transvenous Obliteration’ (CARTO).
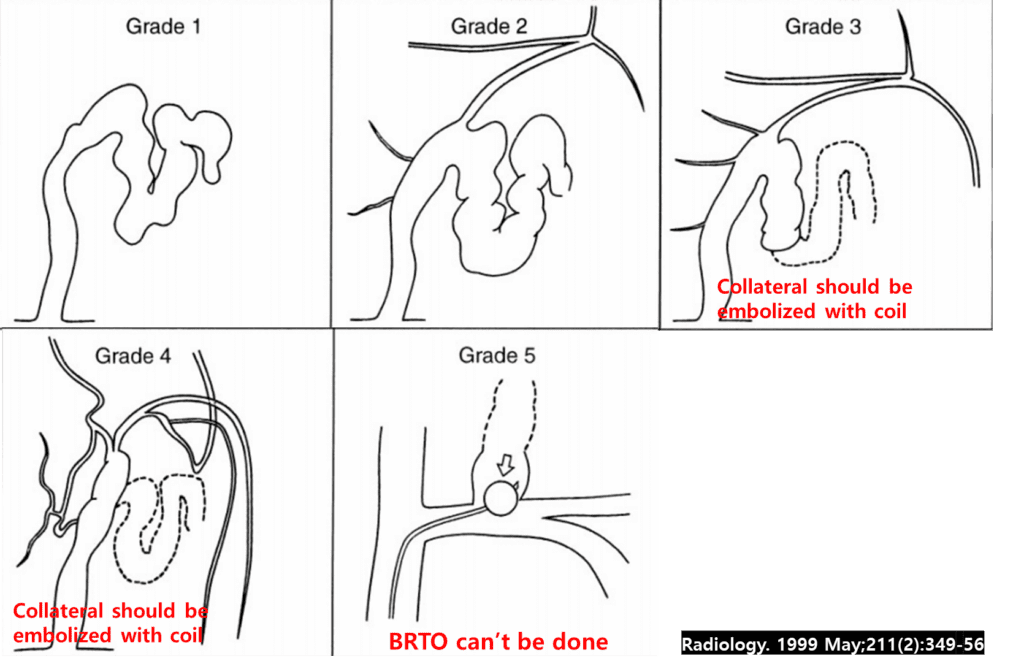
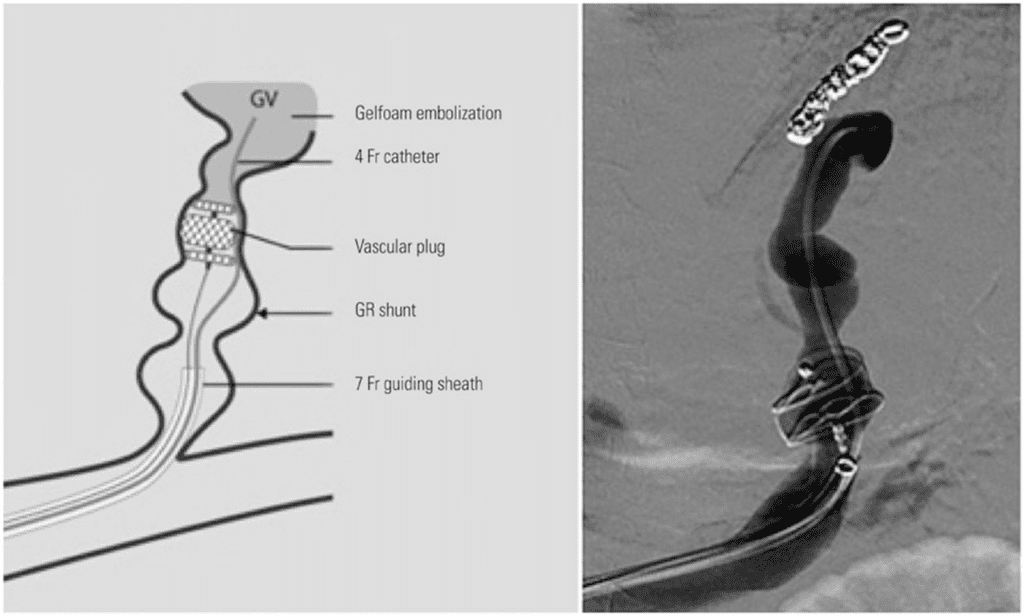
There are similar concepts such as BRTO (Balloon-occluded Retrograde Transvenous Obliteration) and PARTO (Plug Assisted Retrograde Transvenous Obliteration).
In BRTO, a balloon is used to occlude the shunt, while PARTO utilizes a vascular plug for this purpose.
When the size of the shunt is too large (or due to an unfavorable shunt angle) to be occluded by a vascular plug, we can use a coil instead.
Because the procedure occludes a physiological shunt, portal pressure increases post-procedure.
While variceal bleeding and hepatoencephalopathy may improve, portal hypertensive complications can worsen.
The increased portal pressure typically decreases over the course of a month.
Unlike TIPS (Transjugular Intrahepatic Portosystemic Shunt), BRTO (and its variants PARTO and CARTO) do not involve puncturing the liver parenchyma, making it less invasive.
While TIPS does not preserve the patient’s liver function, BRTO can enhance it.
Thus, BRTO (as well as PARTO and CARTO) can be performed on patients with poor hepatic function reserve
- sclerosing agent – minimum 2 hour ballooning should be maintained
Related posts:
 Today’s case 2 – Portal vein stent insertion for invaded main portal vein by pancreas head cancer
Today’s case 2 – Portal vein stent insertion for invaded main portal vein by pancreas head cancer  Today’s case 3 – PICC (peripherally inserted central catheter)
Today’s case 3 – PICC (peripherally inserted central catheter)  Today’s case 4 – Iatrogenic bleeding of deep femoral artery while insertion of A-line
Today’s case 4 – Iatrogenic bleeding of deep femoral artery while insertion of A-line  Today’s case 12 – Successful selective thoracic duct embolization(TDE)
Today’s case 12 – Successful selective thoracic duct embolization(TDE)