Takayasu arteritis
Takayasu arteritis is a chronic vasculitis mainly involving the aorta and its main branches such as the brachiocephalic, carotid, subclavian, vertebral, and renal arteries, as well as the coronary and pulmonary arteries.
It induces clinically varied ischaemic symptoms due to stenotic lesions or thrombus formation. More acute progression causes destruction of the media of the arterial wall, leading to the formation of aneurysms or rupture of the involved arteries.
Almost all patients have ischemic disorders of the involved vessels (mostly cervical lesions in Japan), which present as dizziness, syncope, visual disturbance, faint or absent pulse, or differences in systolic blood pressure between arms.
Takayasu arteritis type IV and giant cell arteritis are vasculitic syndromes affecting the central pulmonary arterial system (large elastic and medium-sized muscular branches).
They are characterized by wall thickening and stenotic changes, which can cause peripheral perfusion asymmetry and arterial thrombosis or thromboembolism with distal pulmonary infarction.
Characteristics of Takayasu arteritis
- F:M = 10:1
- Peak : 3rd decade
- Clinical presentation
- Pre-pulseless phase: nonspecific inflammatory feature
- Fever, night sweats, malaise, weight loss, arthralgia, myalgia
- Tenderness over affected arteries
- Pulseless phase: stenosis, occlusion and aneurysm
- Diminished pulse with limb claudication
- Pre-pulseless phase: nonspecific inflammatory feature
Radiographic findings of Takayasu arteritis
- Ealy stage: acute inflammatory phase
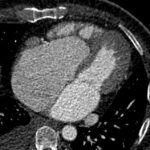
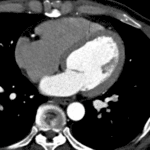
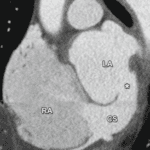
- CT/MRI: vessel wall thickening with enhancement
- PET: increased FDG uptake
- Late stage: healed fibrotic phase
- Angiography: stenosis and occlusion
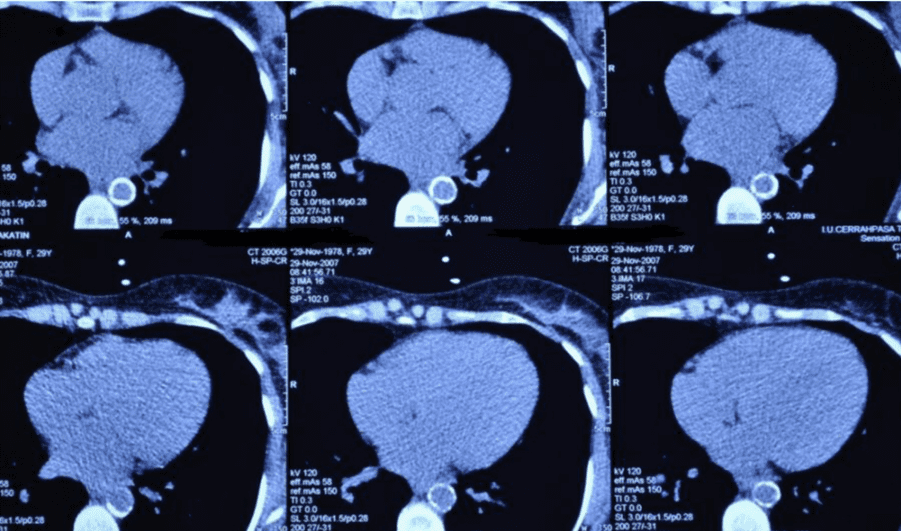
- CT/MRI: stenosis, occlusion and transmural wall calcification
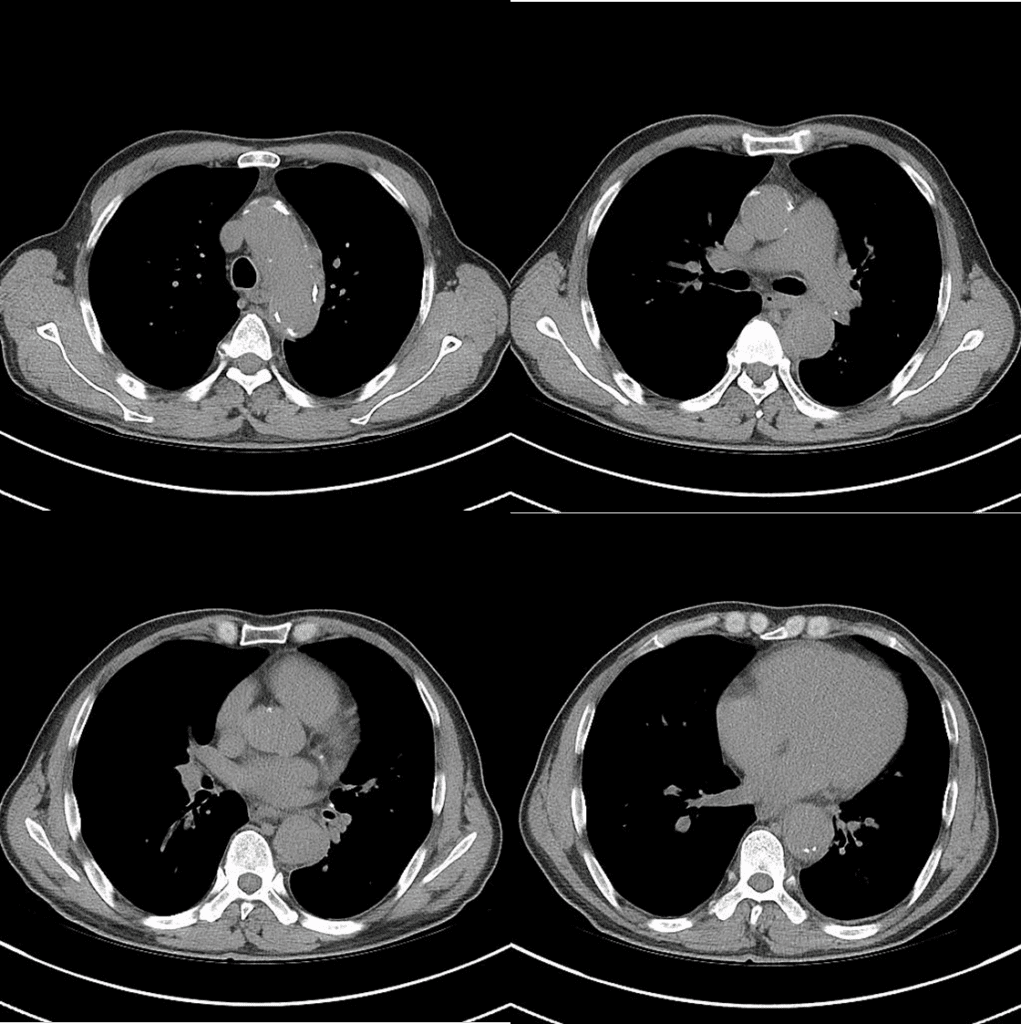
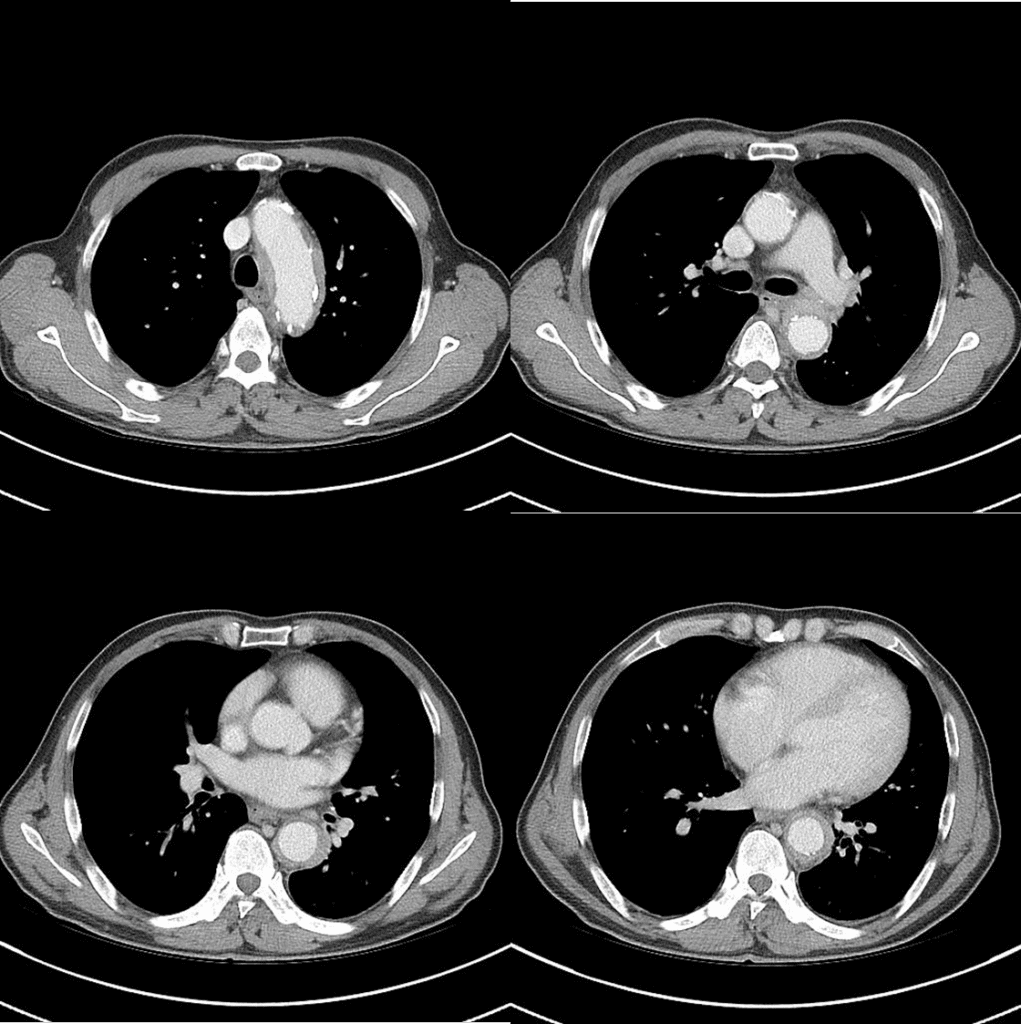
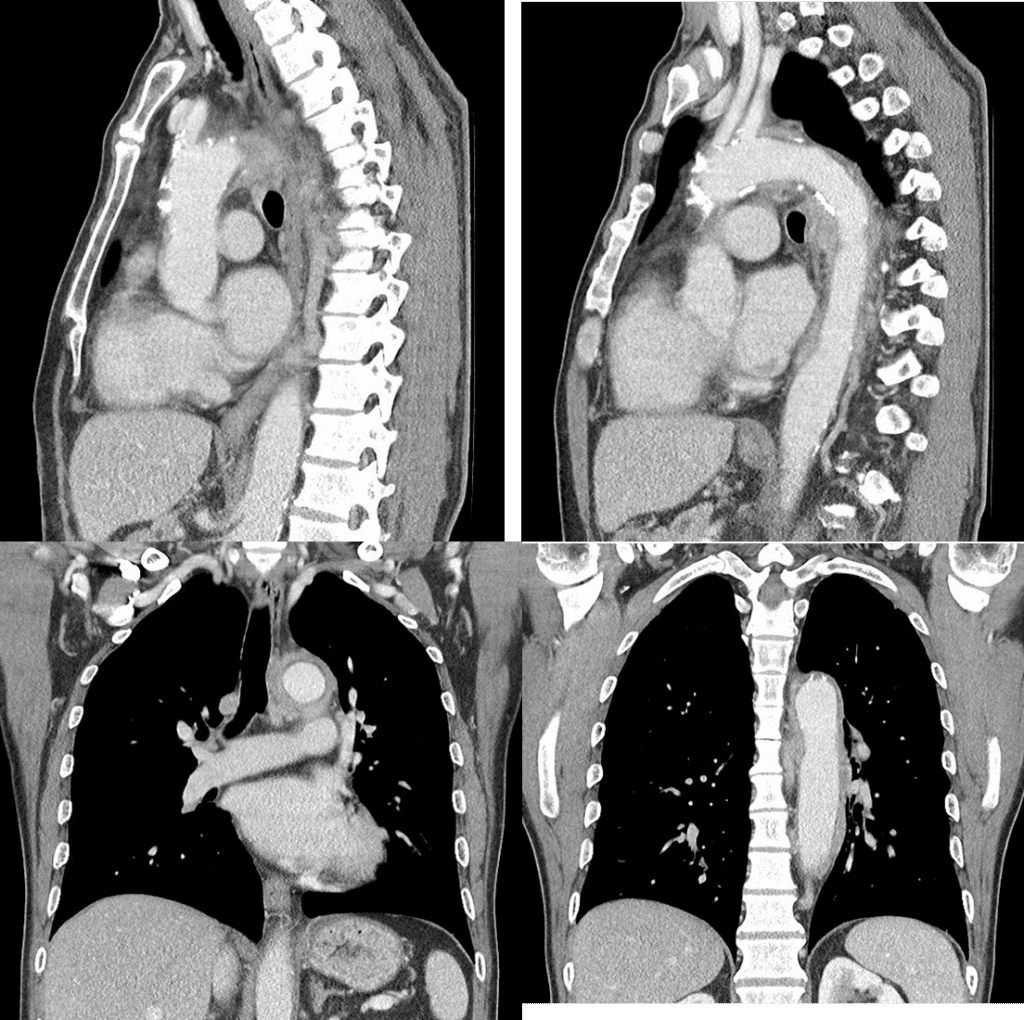
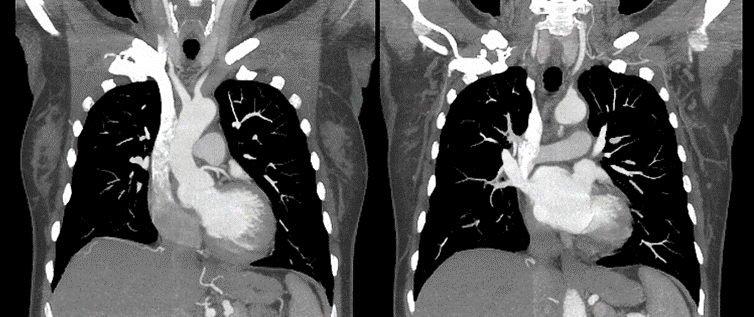
reveals diffuse wall thickening and enhancement of aorta.
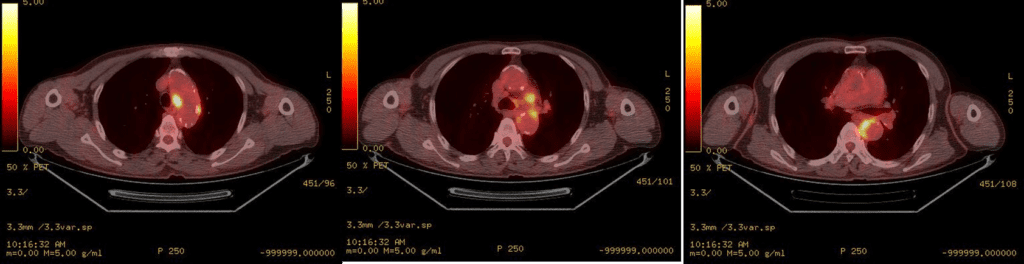
Multifocal hypermetabolic lesions along the aortoc arch, descending thoracic aorta (SUVmax= 9.0), suggesting acute phase of the disease
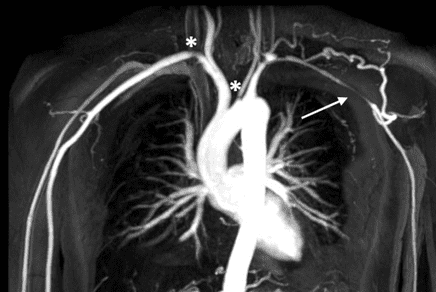
Note that left subclavian artery shows long segmental stenosis (arrow)
- Differential diagnosis
- Giant cell arteritis : usually involves external carotid artery and its branches. headache is common symptom of it
- IgG4 related disease
References)
1. Numano F, Okawara M, Inomata H, Kobayashi Y. Takayasu’s arteritis. Lancet 2000; 356:1023-1025.
2. Engelke C, Schaefer-Prokop C, Schirg E, Freihorst J, Grubnic S, Prokop M. High-Resolution CT and CT Angiography of Peripheral Pulmonary Vascular Disorders. RadioGraphics 2002; 22: 739-764.
3. Dan Longo et al. 2013. Harrison’s Principles of Internal Medicine. 18th Edition.
4. AJR. 2005;184: 1945-1950.10.2214
5. J Clin Pathol. 2002 Jul; 55(7): 481–486.
6. Insights Imaging. 2012 Dec; 3(6): 545–560.
See more about cardiovascular imaging
Follow my instagram