What is the hypertrophic cardiomyopathy (HCMP)
HCMP is defined as myocardial dysfunction resulting from thickening of the left ventricular myocardium, without other systemic cause (e.g., hypertension or aortic valve stenosis).
Thickening is often asymmetrical with involvement of the interventricular septum but may also be diffuse.
Hypertrophic changes result in decreased left ventricular wall compliance as well as left ventricular chamber volume, both of which contribute to diastolic dysfunction.
HCMP
A diffuse or segmental LV hypertrophy (>15 mm on end-diastolic phase) with a nondilated and hyperdynamic chamber in the absence of another cardiac or systemic disease capable of producing the magnitude of hypertrophy evident
Diastolic dysfunction ➜ Later systolic dysfunction
Most common genetic cardiovascular disorder (family screening) in autosomal dominant fashion.
Most common cause of sudden cardiac death in young people
Histology : Myocardial disarray as well as patches of myocardial scarring
Treatment : Ablation or mymectomy
The main purpose of MRI
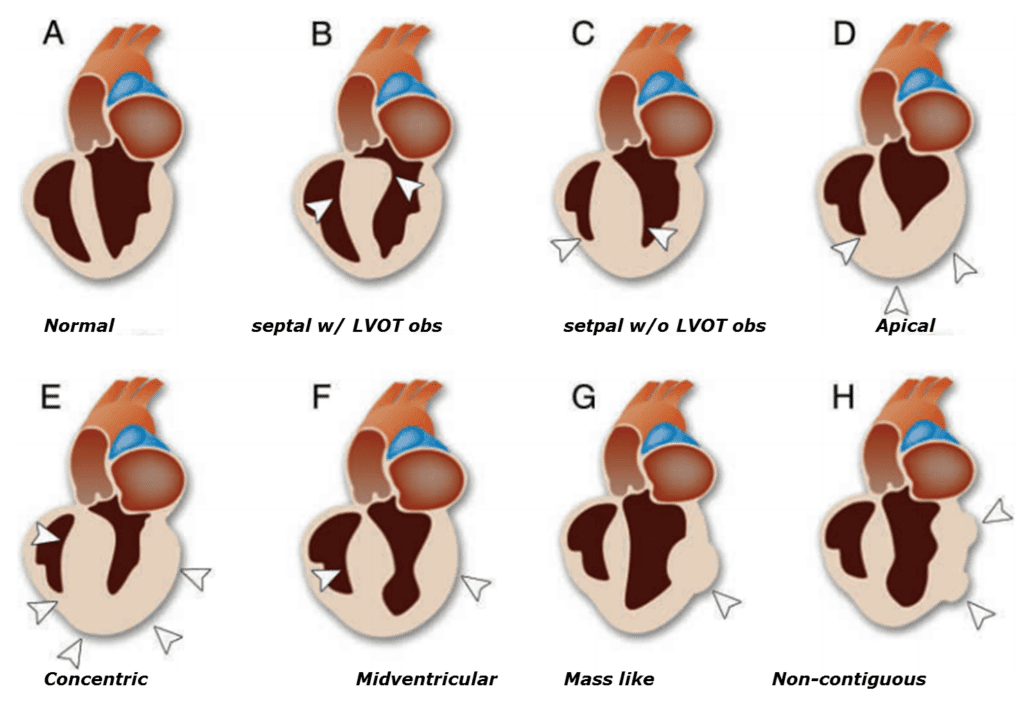
– To determine the phenotypes
– Assessment of cardiac function and evaluation of dynamic obstruction
– Risk stratification (demonstration of myocardial scarring and fibrosis)
; Guide of therapy such as septal ablation
MR diagnostic criteria
– LV wall thickness > 15mm at end-diastolic phase
– Wall thickness ratio > 1.3-1.5 at apex
Risk stratification (high risk of sudden death)
– LV wall thickness ≥ 30mm at end-diastolic phase
– LVOT gradient ≥ 30mmHg
– Apical aneurysm
– LV dilatation with depressed EF (end stage HCMP, EF <50%)
– Perfusion defect
– Late enhancing areas with DE-MRI
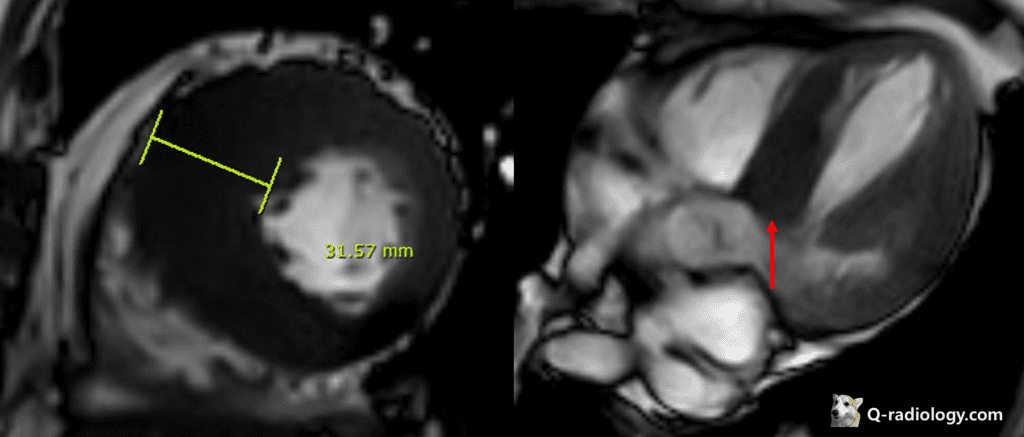
Note that more than 30mm ventricular wall thickening is a risk factor for sudden cardiac death
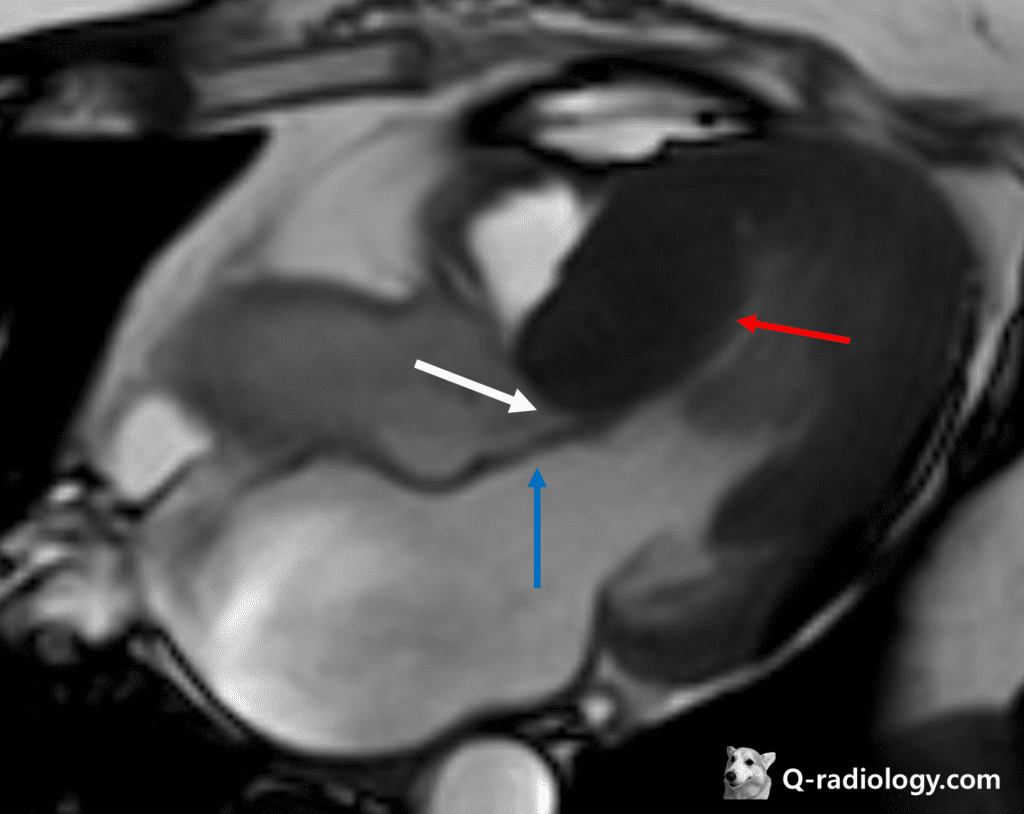
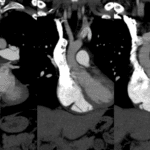
Blue arrow : systolic anterior motion
White arrow : LVOT obstruction
Septal type HCMP with systolic anterior motion(SAM) and associated LVOT obstruction
Mitral regurgitation is also seen
•ASH (asymmetric septal hypertrophy)
•SAM (systolic anterior motion) of the mitral valve
•LVOT obstruction (20-30%) and MR (mitral regurgitation)
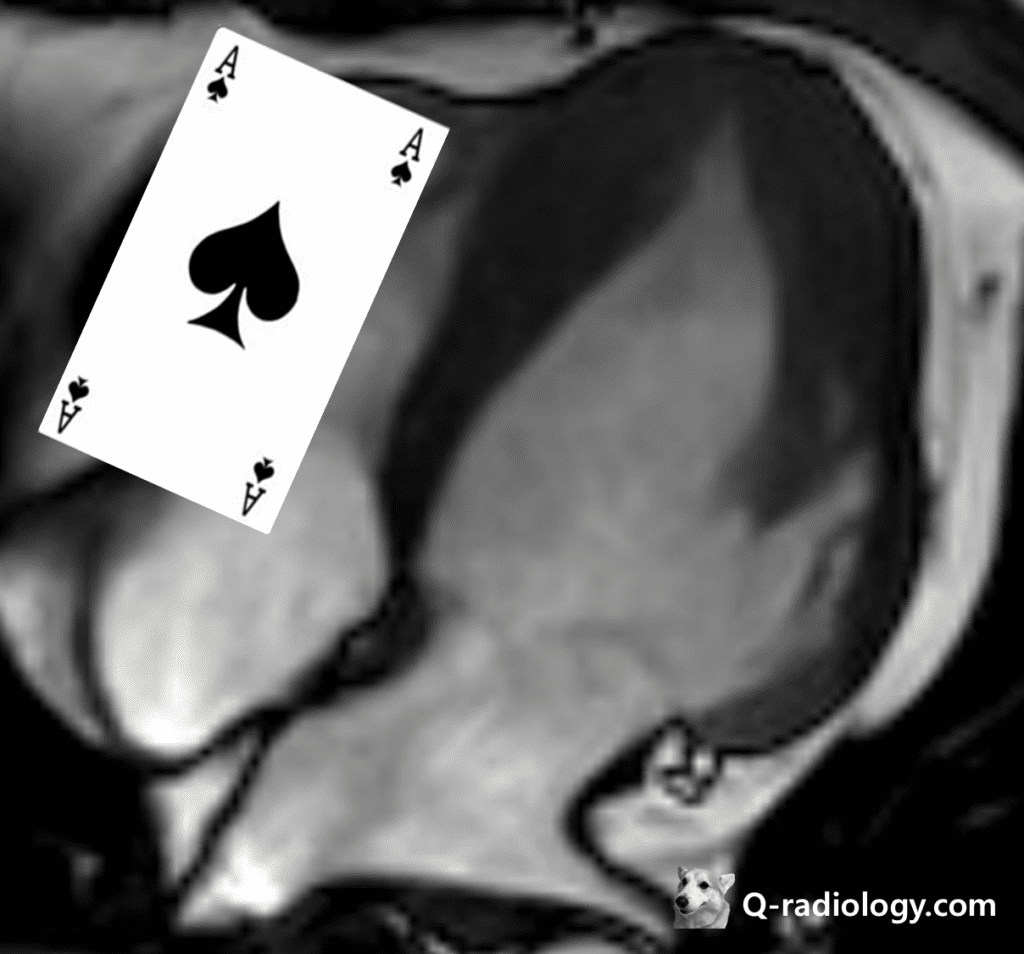
Apical HCMP
– common in Asian middle-aged male, might be missed on EchoCG (Giant T-wave inversion)
– myocardial hypertrophy (“Spade Ace sign”) at apex & apical segment
– Diagnostic criteria: absolute apical wall thickness of > 15 mm or a ratio comparing apical LV and basal LV wall thickness of 1.3-1.5
Burned-out phase of HCMP
End stage of HCM
– Systolic dysfunction
– LV dilatation and wall thinning
– Transmural enhancement (myocardial fibrosis)
– Unfavorable outcome
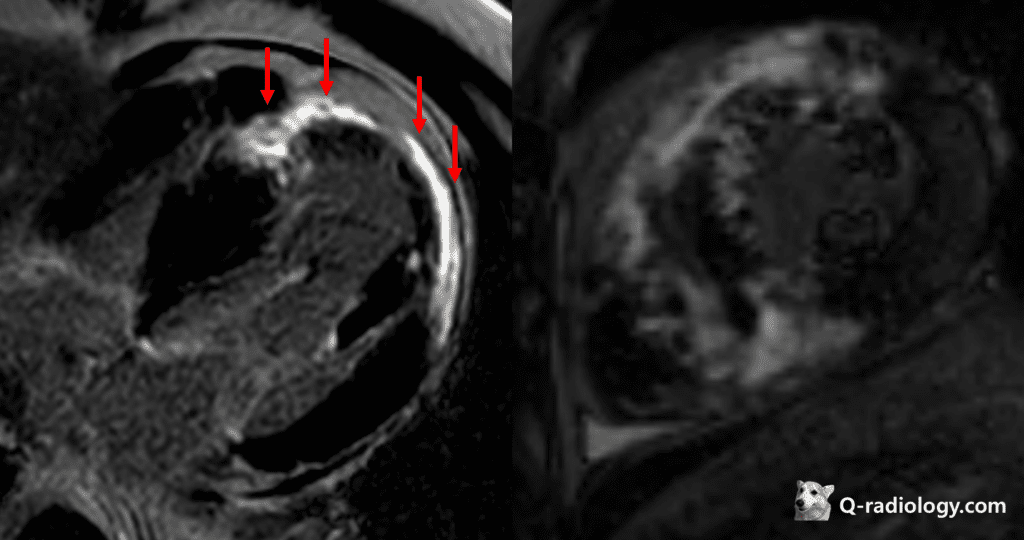
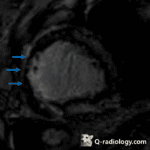
Subepicardial patchy DEs at LV mid septal/anterior/apical entire wall, myocardial fibrosis with LV septal wall thickening, suggestive Burned-out phase of HCMP
Reference)
Charles S. White, Linda B. Haramati, Joseph Jen-Sho Chen, and Jeffrey M. Levsky (2014), Cardiac Imaging, Oxford university press