A. High risk lesions
- 1) Atypical ductal hyperplasia
- Location: terminal duct lobular unit and terminal duct
- Proliferation of evenly distributed, monomorphic cells
- Appropriate management: surgical excision
- 2) Lobular neoplasia
- Atypical lobular hyperplasia
- Lobular carcinoma in situ
B. Borderline lesions
- 1) Atypical papilloma, Papillary lesion
- Risk and management
- Central < Peripheral < Atypical papilloma
- Benign papilloma ; variable, but surgical excision in case with larger size and peripheral location
- atypical papilloma : 7 times higher risk and surgical excision is needed
- Imaging finding * MG ➜ US ➜ Ductography
- MG – circumscrbed oval mass, calcification
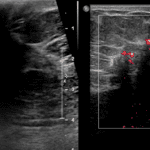
- US – complex echoic mass, ductal dilatation with intraductal solid mass
- Risk and management
- 2) Radial scar
- Idiopathic, not related to prior surgery or trauma
- Fibroelastic core with entrapped ducts and surrounding radiating ducts and lobules
- Surgical excision
- Imgaing finding
- MG – asymmetric density or architectural distortion with central translucent area / spiculation with central lucency
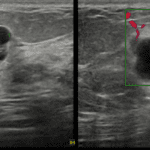
- US – irregular hypoechoic mass with strong posterior acoustic shadowing
- 3) Mucocele like lesion
- Multiple cysts containing mucin with extravasation into the stroma
- Imaging finding
- MG – isodense mass with or without calcification
- US – Ill-defined aggregated cysts and distended ducts with or without mural calcification
- Excisional biopsy is required
- 4) Phyllodes tumor
- 5) Flat epithelial atypia (Columnar cell lesion with atypia)
- Normal breast are consisted with cuboid cell and the cells changes into columnar cell, this process is called columnar cell change
- Columnar cell change itself is not harm, but with atypia is its called flat epithelial atypia (Need excision)
- Imaging findings
- MG – Amorphous (65%), coarese heterogenous, finer pleomorphic, grouped
- 6) Sclerosing adenosis with atypia