A 74-year old female showed abnormal hypercalcemia on pre-operative lab (she was scheduled to have TKRA)
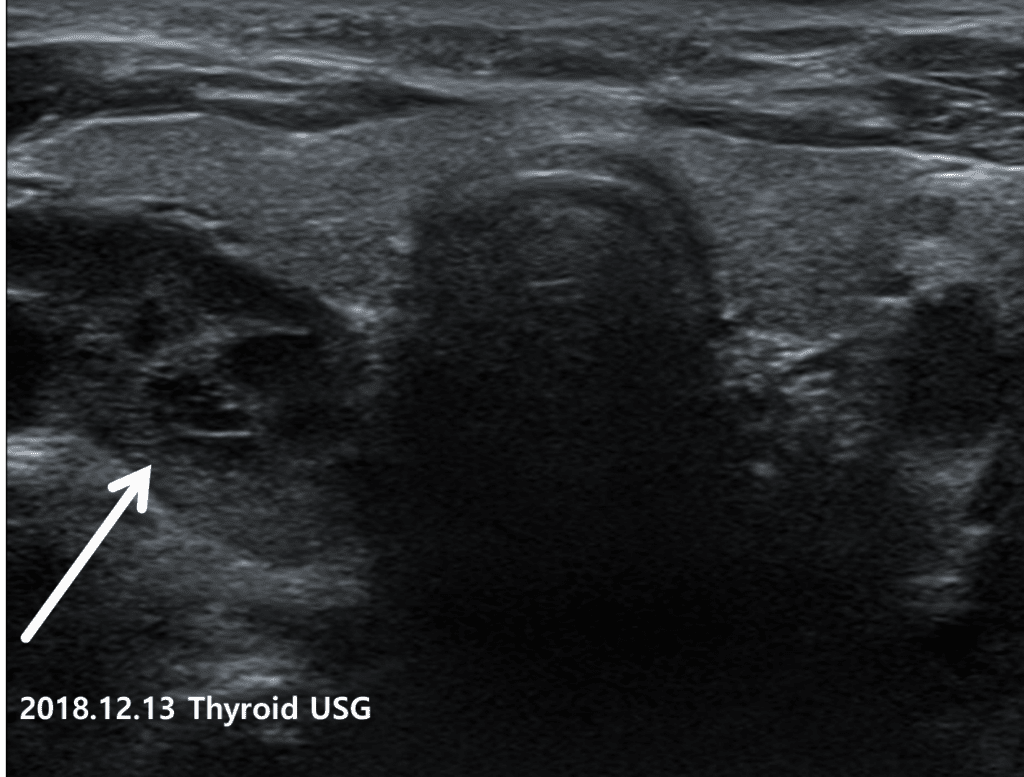
Neck sonography was asked to rule out primary hypercalcemia
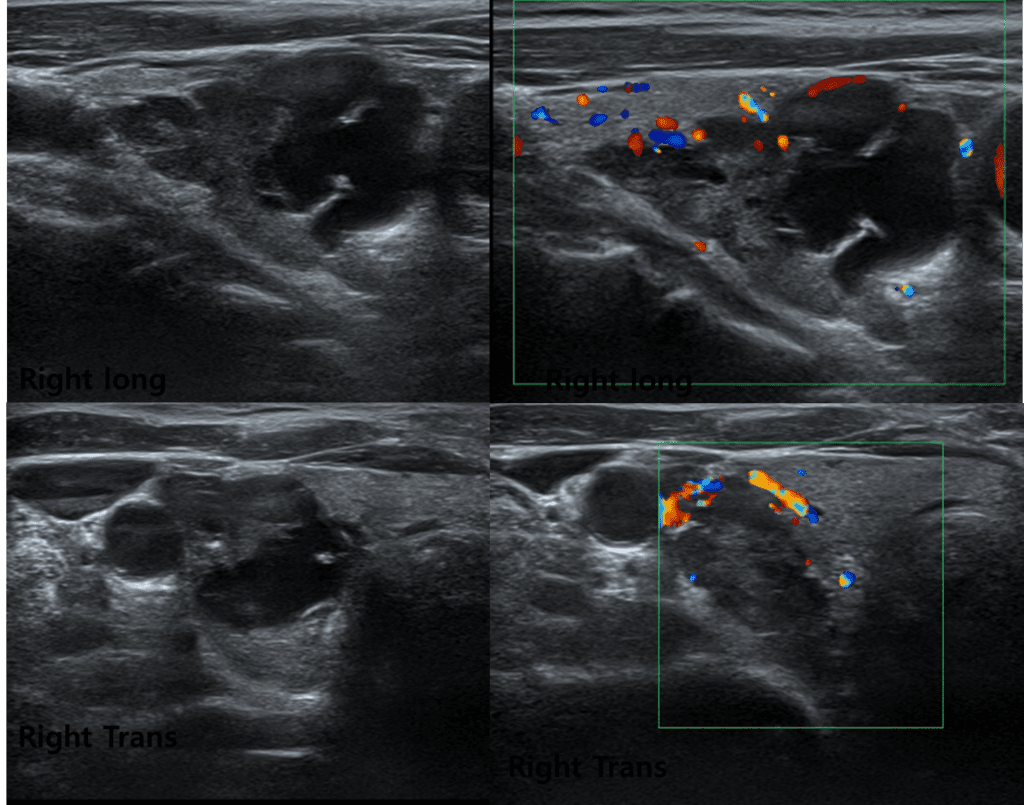
Color doppler image shows ‘polar feeding artery’
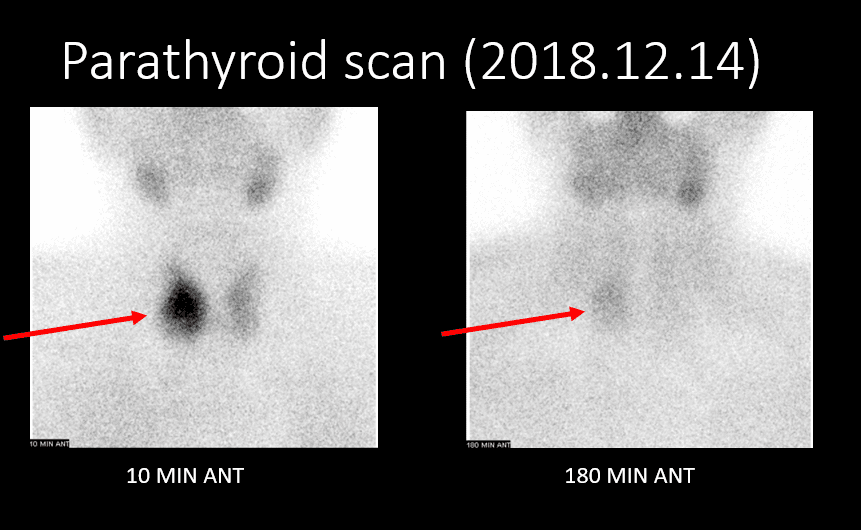
delayed image shows hot uptake at right parathyroid gland
the location of the lesion well correlates with ultrasonography
- Parathyroid gland
- 35-40mg
- Yellow
- Supplied from end artery (esp. ITA branch)
- Inferior parathyroid gland – 3rd branchial pouch ; long migration path makes more ectopic location of it
- Superior parathyroid gland – 4th branchial pouch
- Parathyroid adenoma is a benign tumor of the parathyroid gland and the most common cause of primary hyperparathyroidism
– The cause of primary hyperparathyroidism ; Parathyroid adenoma (80-85%), primary parathyroid hyperplasia (15%), parathyroid carcinoma(5%)
- Clinical presentation
- Non-specific symptoms (fatigue, weakness)
- Elevated serum calcium levels and elevated serum parathyroid hormone levels
- Elevated serum calcium levels and elevated serum parathyroid hormone levels
- Non-specific symptoms (fatigue, weakness)
- US features
- Hypoechoic solid mass with oval, bean-like or multilobulated shape
- **cystic degeneration in 2%
- Color or power Doppler US
– Polar feeding artery to one pole generally from inf. thyroidal artery
– Location Posterior or inferior to thyroid gland
- Nuclear medicine
- 99mTc-sestamibi SPECT (photon energy: 140 KeV)
– Diffuse passively across cell membrane, concentrate in mitochondria - Parathyroid adenomas are best demonstrated on delayed imaging (1-2 hours)
- 99mTc-sestamibi SPECT (photon energy: 140 KeV)