Liver abscess percutaneous drainage case (Hepato-venous fistula)
A 40-year-old male undergoing cancer treatment for pancreatic cancer due to pancreas cancer presented to the emergency room after experiencing a fever for three consecutive days.
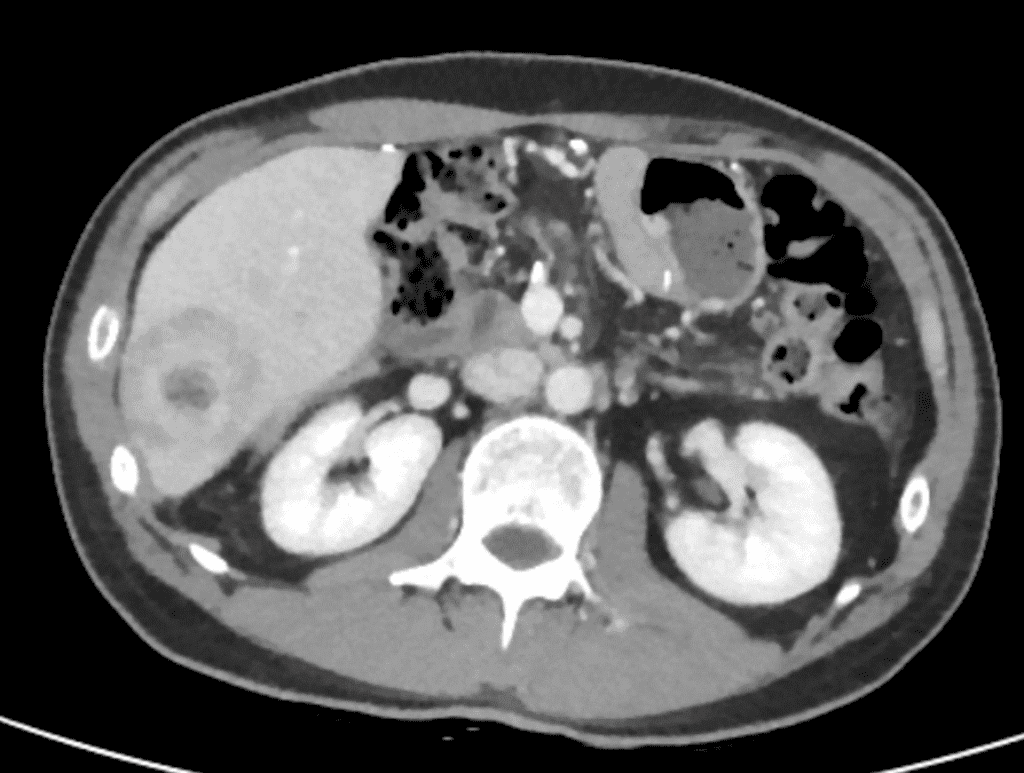
A CT scan revealed the presence of abscess formation with a double target sign in segment 6 of the liver.
The patient was referred to angioroom to insert percutaneous drainage tube into the abscess cavity
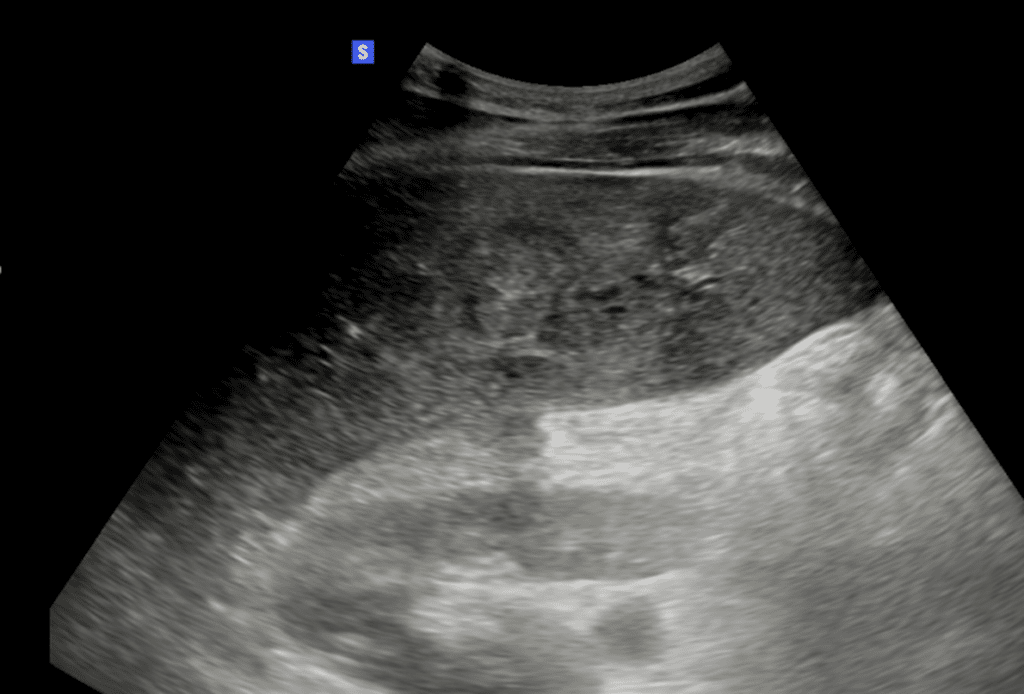
On Ultrasonographic guidance, I punctured the abscess cavity using a Chiba needle (21G)
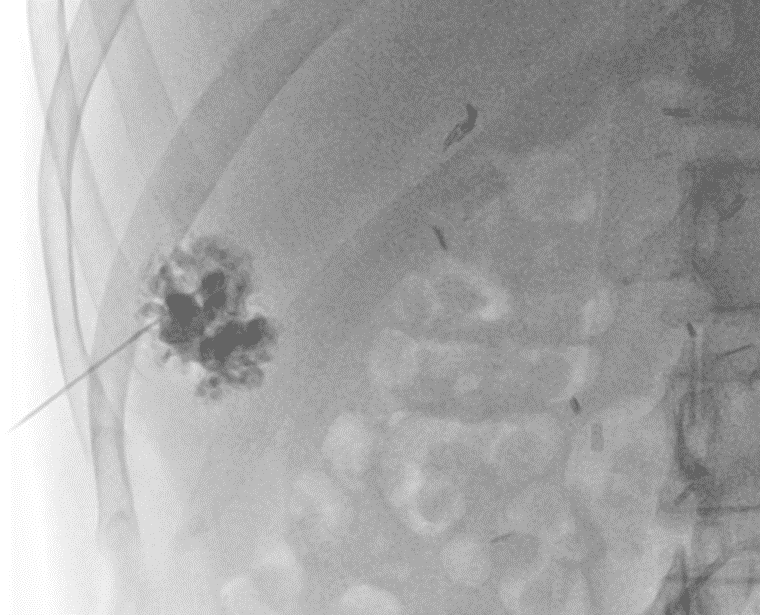
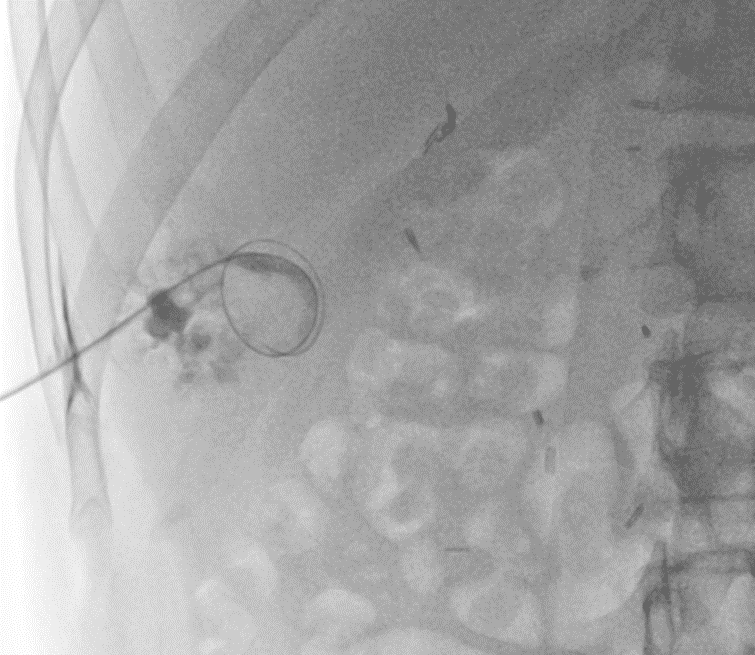
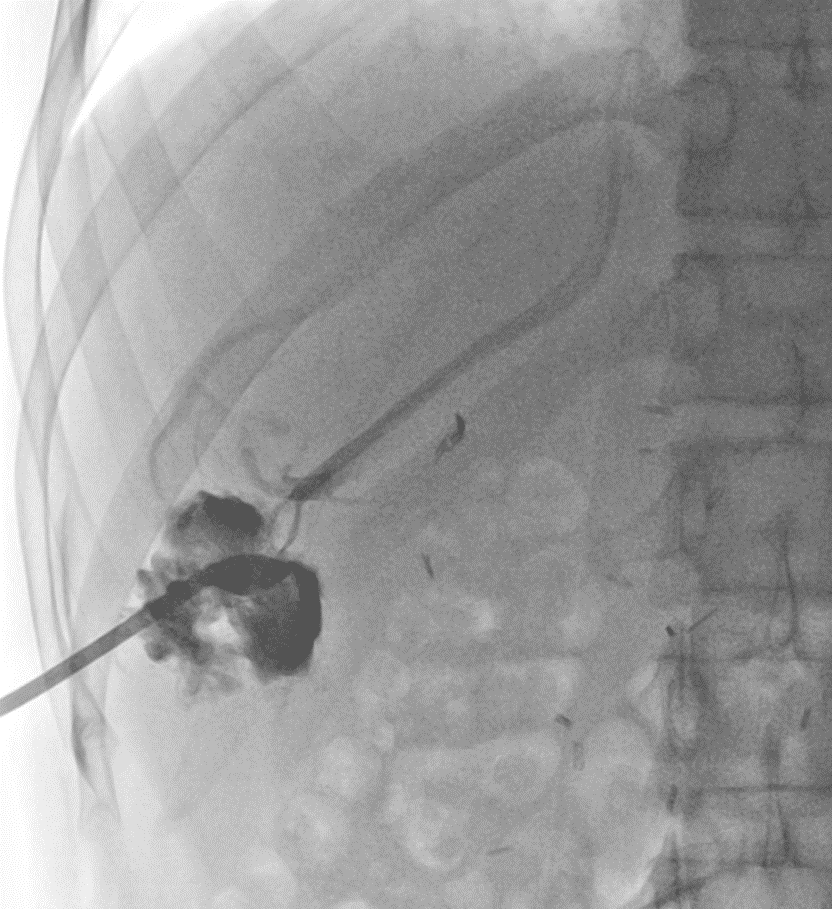
Venous blood was observed flowing from the tube.
Therefore, we advised the clinical team to clamp the tube for approximately two days, and after confirming no bleeding after this period, we informed them that it was acceptable to commence drainage.
I searched for other cases related to liver abscesses connected to vascular structures and found a relevant case report.
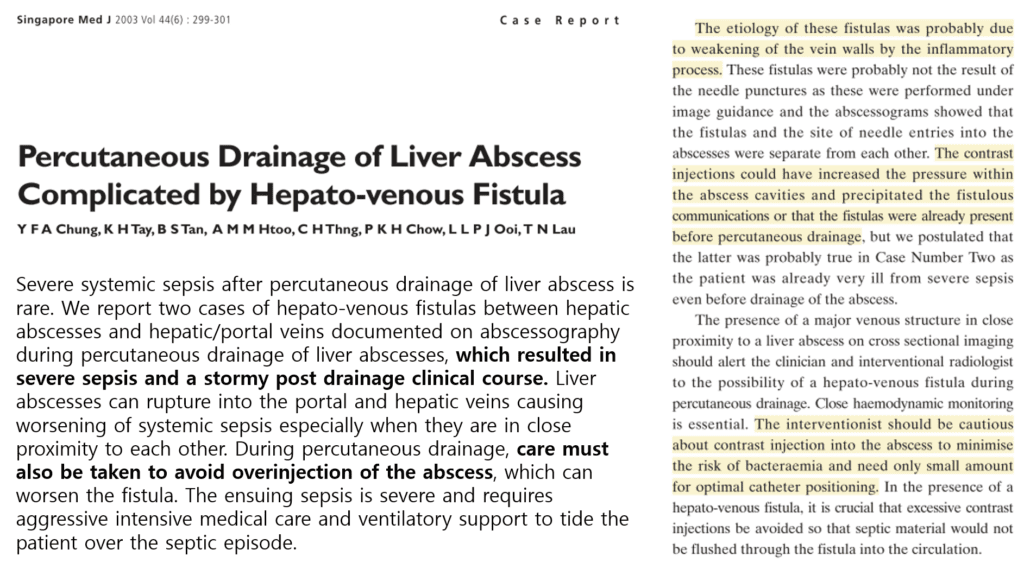
What’s important to note is that systemic sepsis can be induced through this pathway.
Therefore, when initially inserting a drainage tube into the abscess, it’s advisable to minimize or only use contrast injection when absolutely necessary.
