TACE for HCC patient Today’s case -1–
69 year old patient with HCC, the patient have had RFA once and SABR to S8 marginal recurrence (‘21.9.23.- ‘21.10.5.).
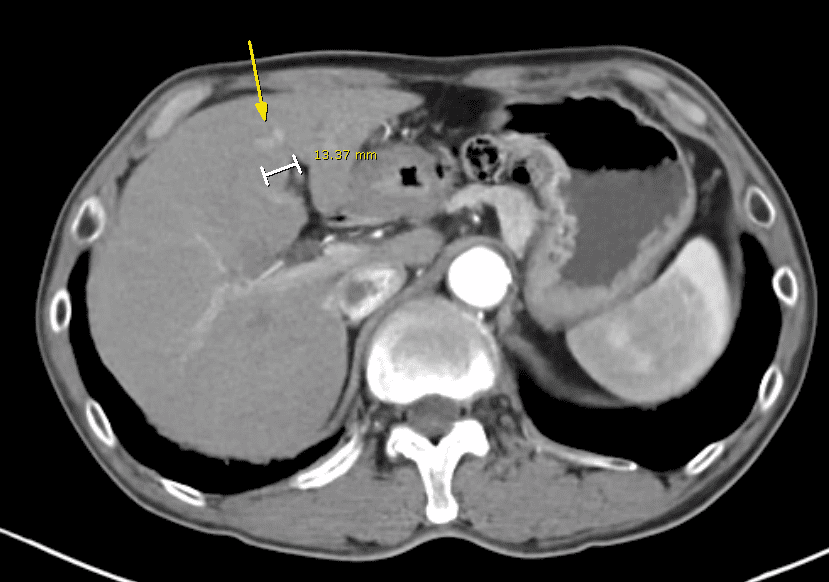
On follow up Liver CT, a nodular lesion is identifed which shows APHE and delayed washout.

The patient refered to angio room for TACE
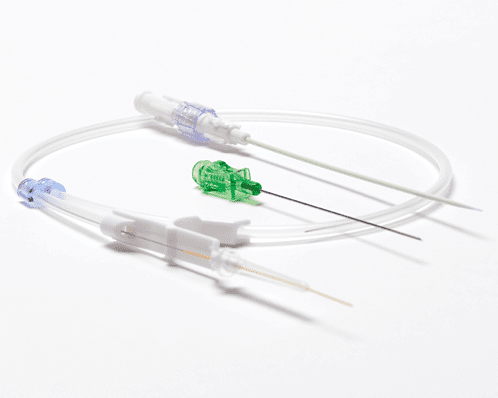
I punctured the patient’s right femoral artery on US guide using micropuncture set

After puncturing the right femoral artery, I inserted a 5Fr sheath. Subsequently, I inserted a 5Fr RH catheter to select the celiac artery.
However, the RH catheter shaping failed due to the patient’s excessive height. I attempted to select the contralateral iliac artery or renal artery to shape the RH catheter, but these attempts also failed. (Our angio room typically uses RH catheters from a Korean company, which often present these kinds of problems.)
Consequently, I requested a longer RH catheter from Cook, as their RH catheters are approximately 5cm longer.
Despite these challenges, I eventually succeeded in shaping the RH catheter using the right renal artery.




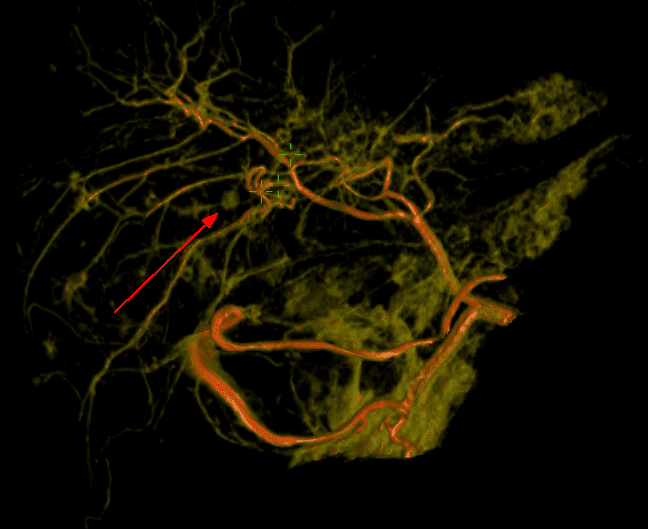
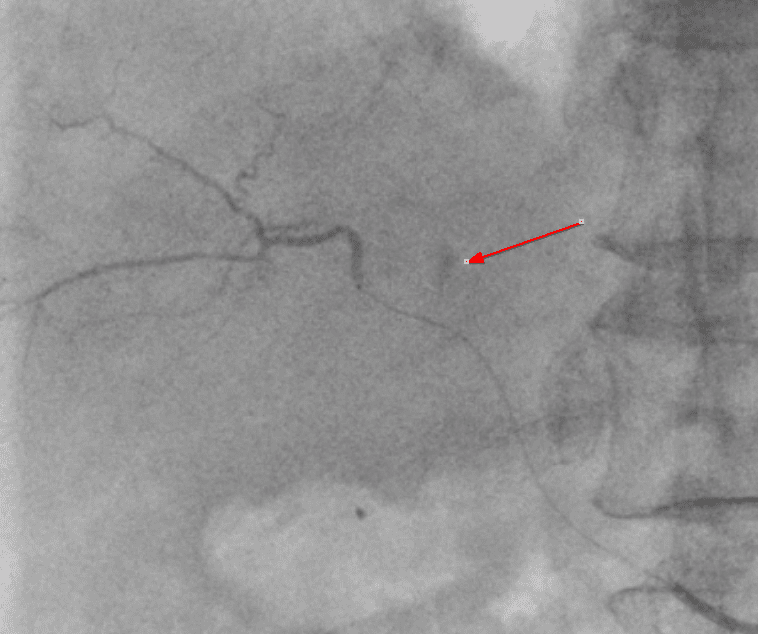
Utilizing these guidance techniques, I attempted to select the feeding artery with a microcatheter (Radiostar microcatheter, 1.9Fr, 110cm) and a microguidewire (ASAHI Meister, 0.016″, 135cm).
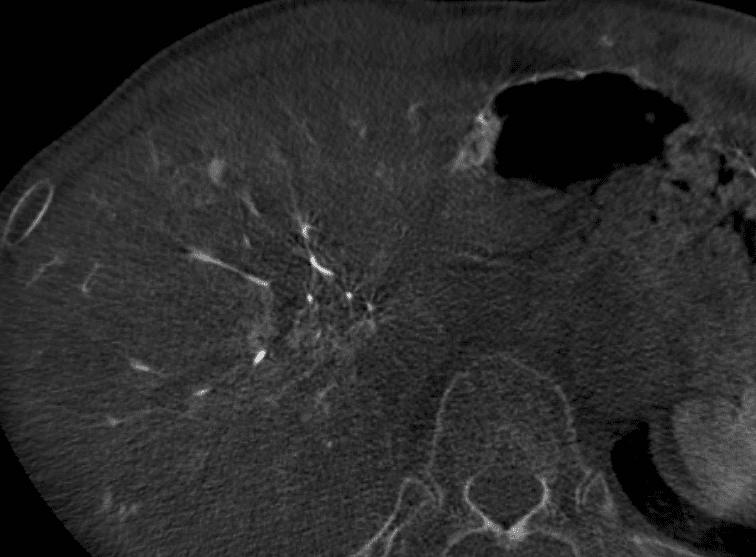
After selecting a small vessel, I checked whether it was the correct vessel using contrast media. However, I did not withdraw blood before injecting the contrast media. Consequently, the following issue occurred…




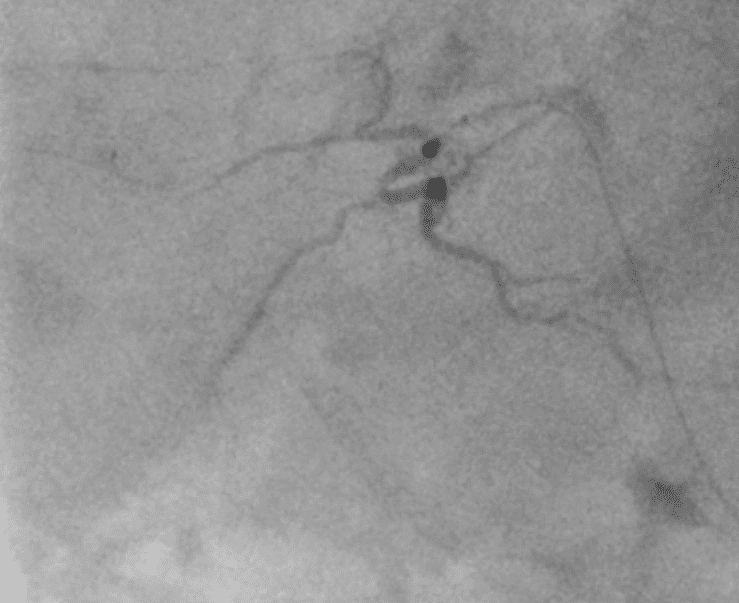



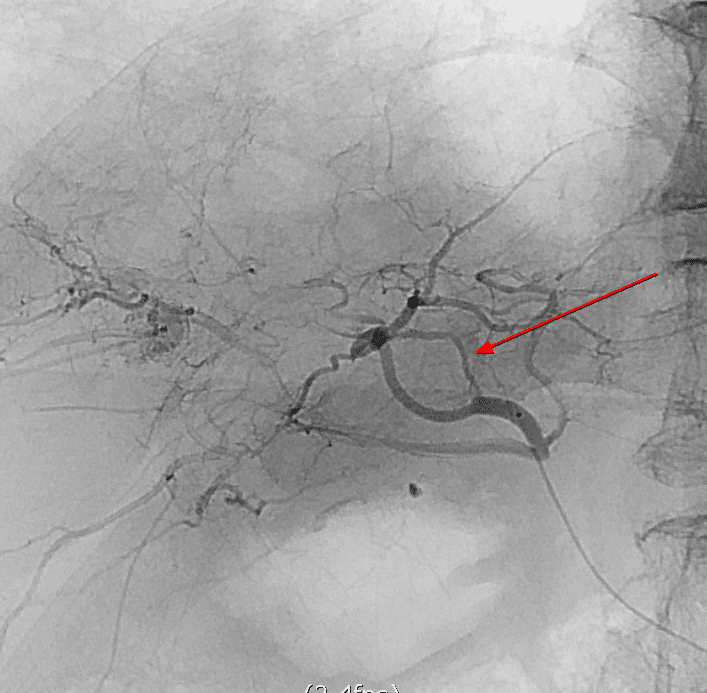
This case provided me with valuable experience, emphasizing the importance of being cautious with the vulnerability of small vessels when using a microcatheter and guidewire.
End of Today’s Case -1-




