Portal vein stent insertion for invaded main portal vein by pancreas head cancer
The patient, who is currently undergoing palliative FOLFIRINOX chemotherapy for inoperable pancreatic cancer with liver metastasis and lymph node involvement, was admitted for elevated liver function tests (LFTs). A CT scan was performed, and upon review by the designated professor in the radiology department, it was noted that there is minimal biliary dilatation. The professor suggested that the elevated LFTs could potentially be attributed to compromised liver perfusion due to portal vein tumor thrombosis (PVTT).
Accordingly, portal vein stent insertion was requested through intervention on radiologic guidance.
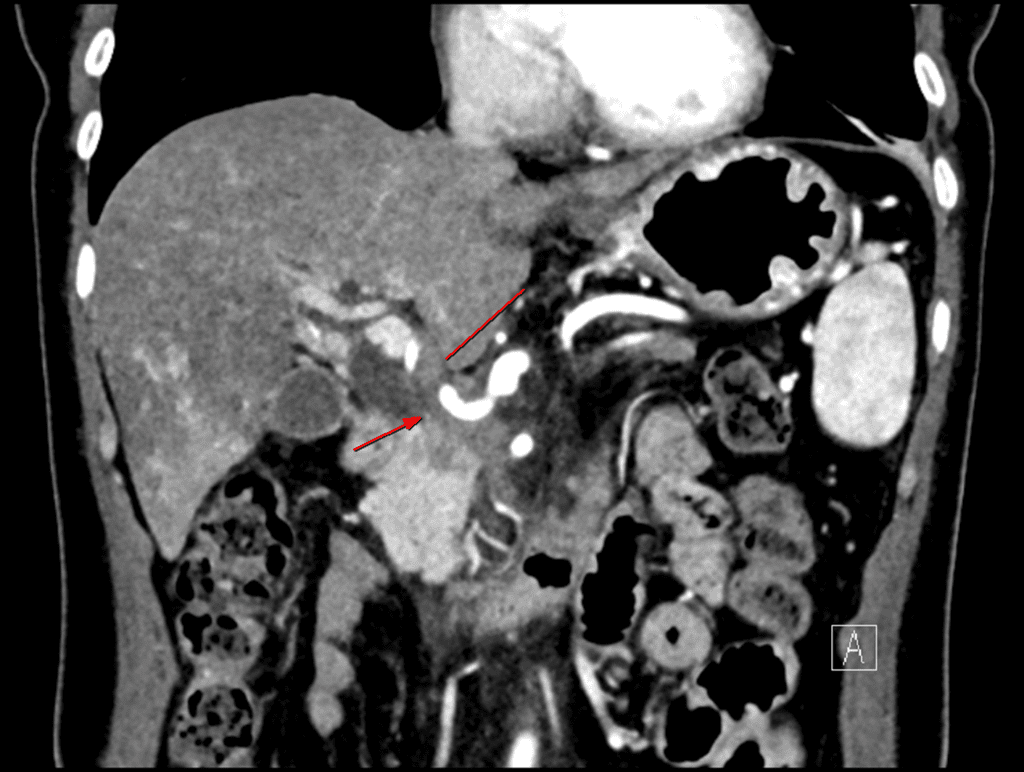
Coronal CT scan shows severe focal stenosis of main portal vein. While not clearly visible in this section, cavernous transformation had developed extensively around the stenotic segment.
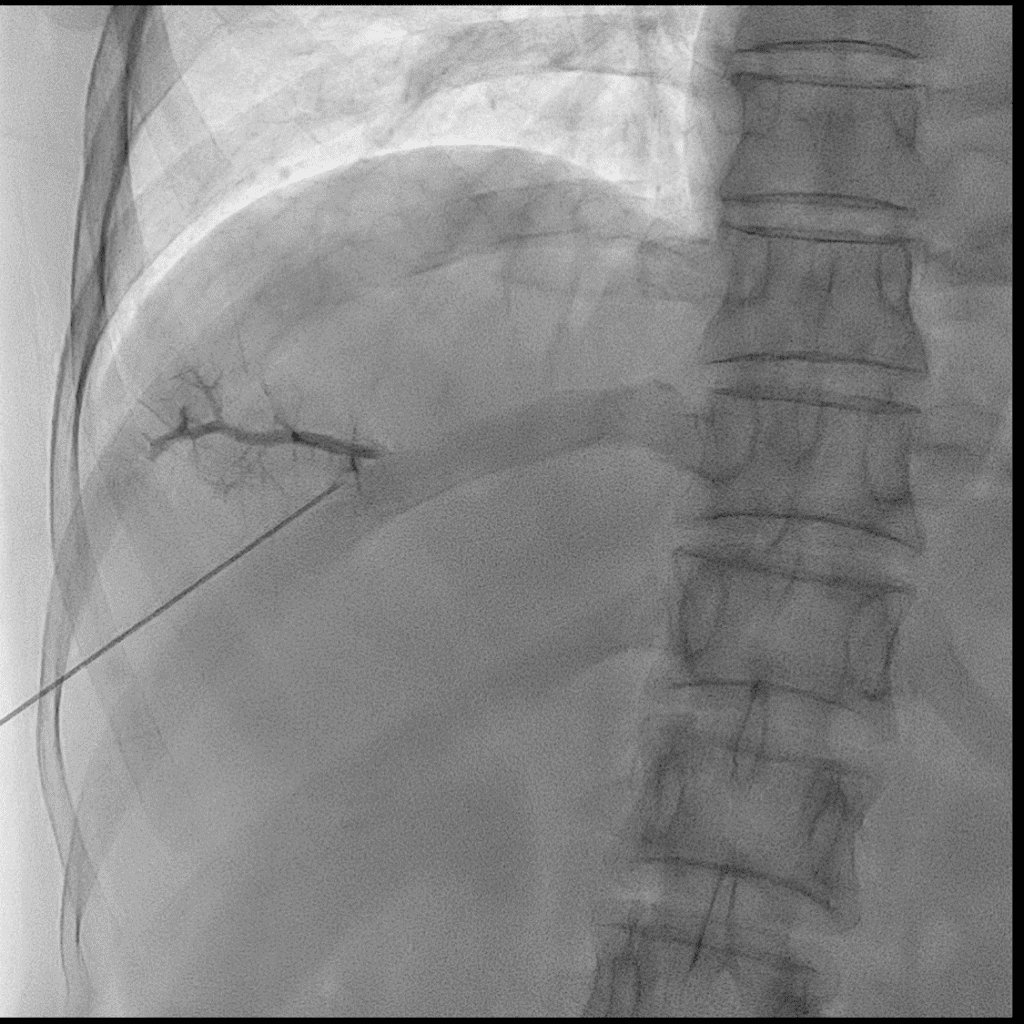
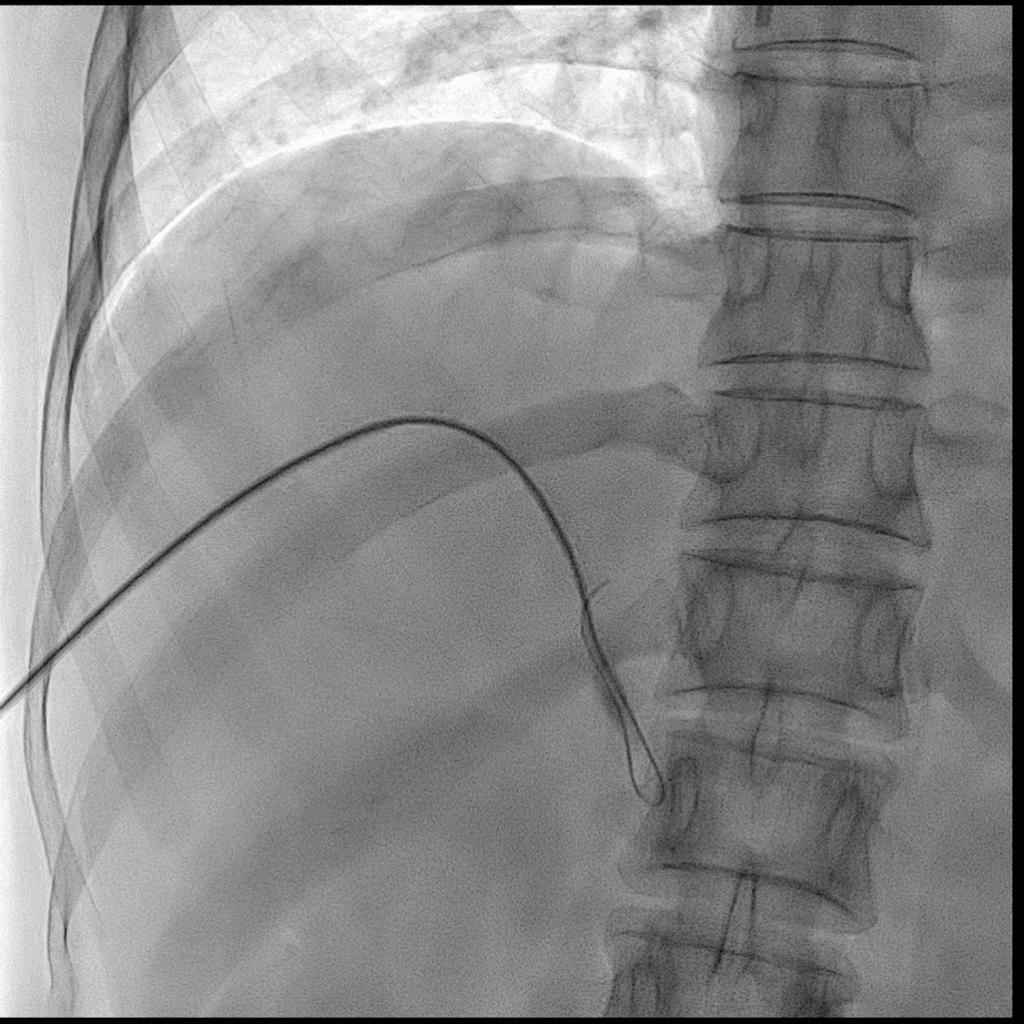
Using a US-guided Chiba needle, puncture was made at P5, followed by insertion of a 5Fr 10cm sheath.
Through the Chiba needle, a guide wire was successfully advanced into the portal vein.
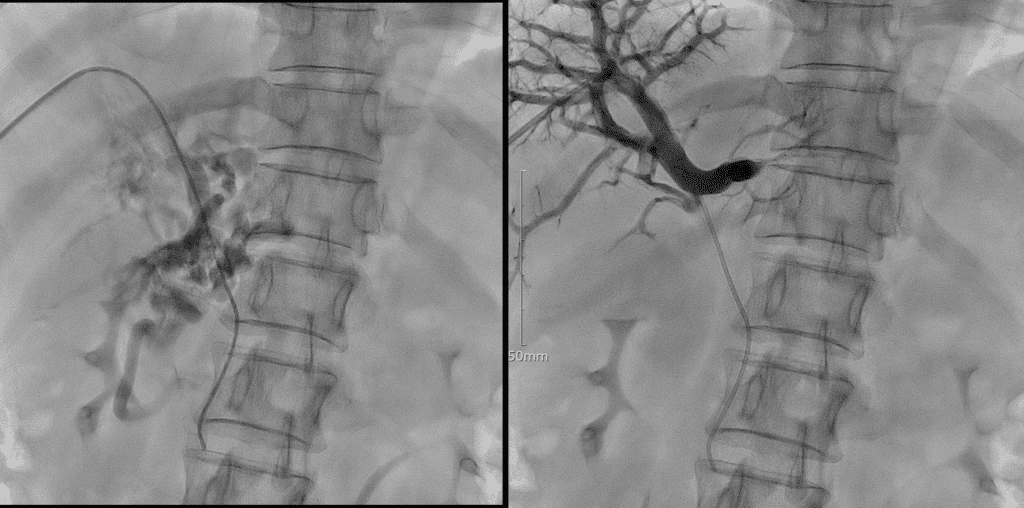
Following the guide wire, a yellow sheath was inserted, and the appearance of the portogram performed through the yellow sheath is shown.
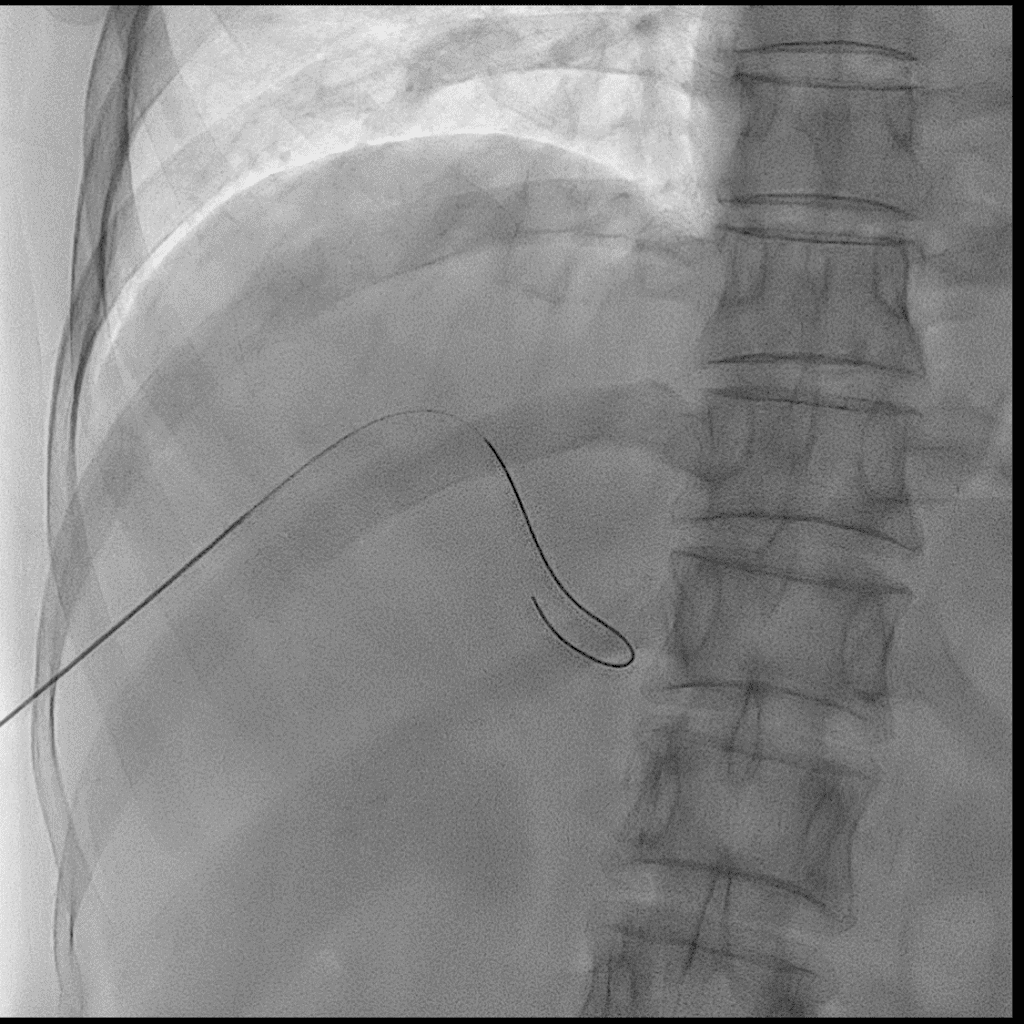
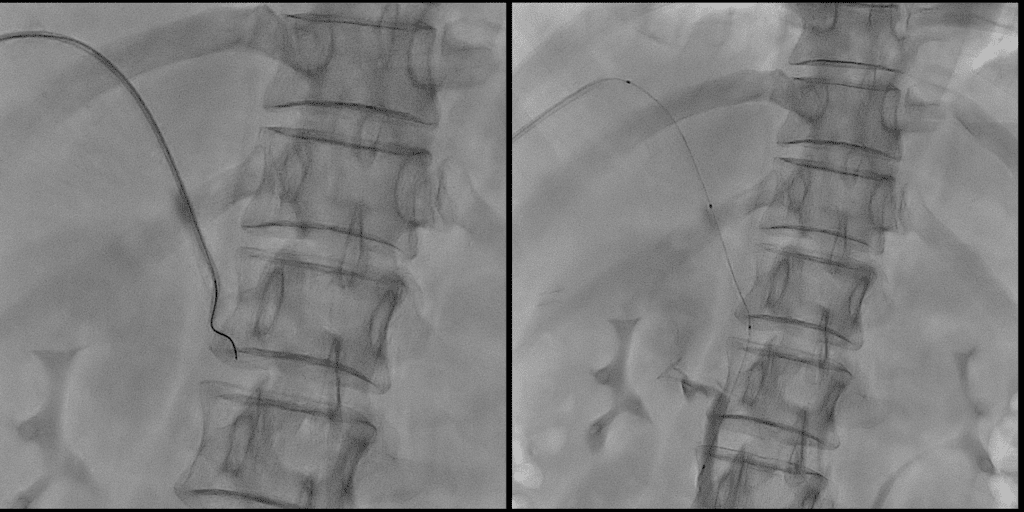
Attempt to pass through the stenotic segment of the MPV using a 40cm KMP and a 0.035″ 150cm guide wire was unsuccessful. At the occluded point, the guidewire couldn’t pass through and exhibited a U-shaped bend.
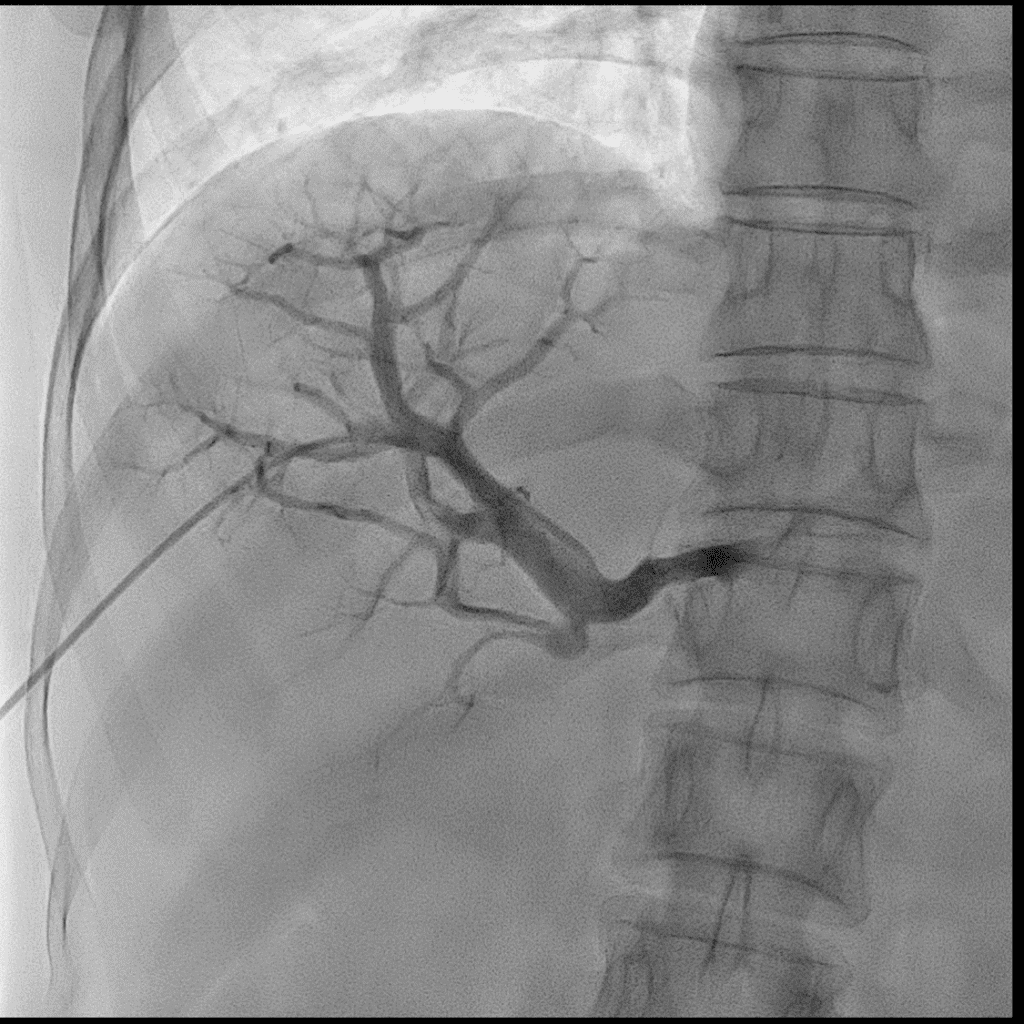
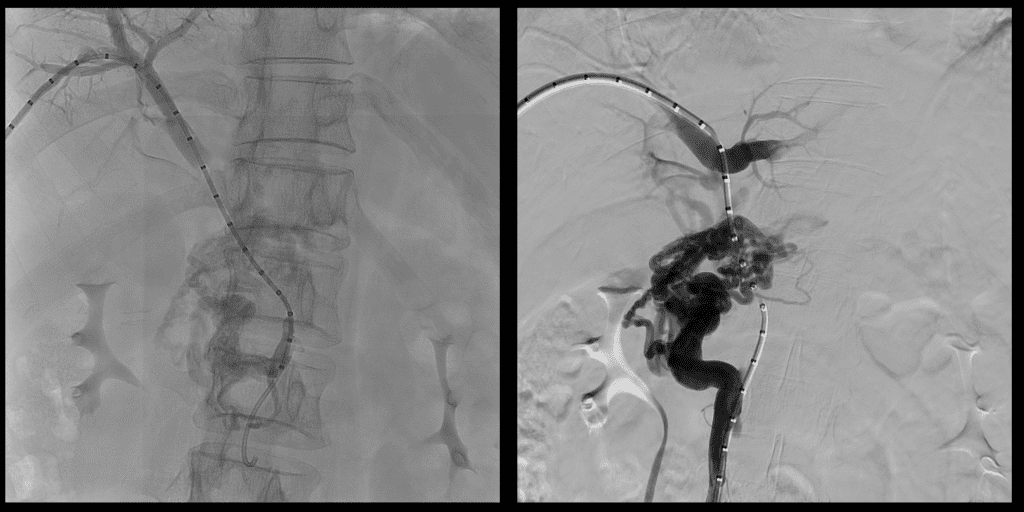
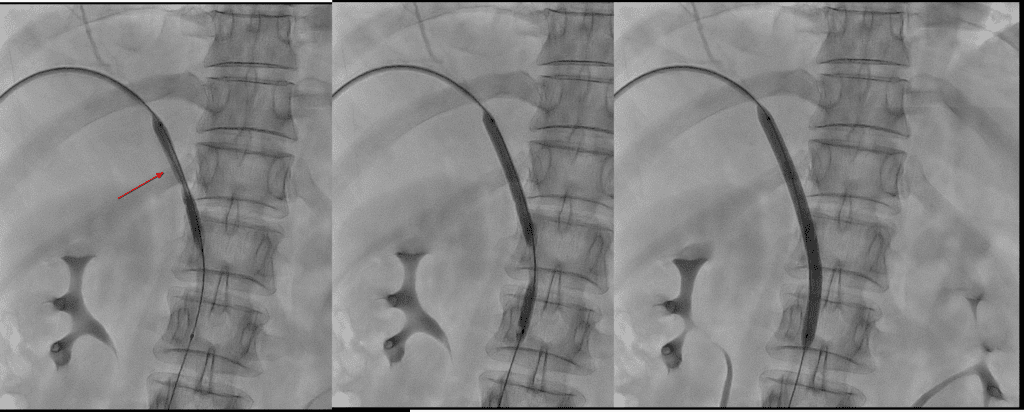
Passage was achieved in traversing the stenotic segment of the MPV using a CXI (90cm) microcatheter and a Command ST (0.018″, 210cm) microguidewire.With the guidewire still in place, the catheter was exchanged to a 4Fr 65cm Davis catheter, and then the guidewire was swapped to a 0.035″ J-tip guidewire (260cm).Next, a measuring pigtail catheter was inserted to gauge the length for stent placement. After measuring, the sheath was exchanged to a 6Fr 10cm one, and pre-dilation of the stenotic segment was carried out using a 6mm x 10cm Mustang balloon (75cm) through the sheath.Next, a measuring pigtail catheter was inserted to gauge the length for stent placement. After measuring, the sheath was exchanged to a 6Fr 10cm one, and pre-dilation of the stenotic segment was carried out using a 6mm x 10cm Mustang balloon (75cm) through the sheath.Next, the sheath was replaced with a 6Fr 25cm one. Two EPIC NITINOL VASCULAR STENT SYSTEMs (12mm x 60mm x 75cm) were deployed with overlap in the stenotic segment of the MPV. Subsequently, post-stent ballooning was performed using a 10mm x 8cm Mustang balloon (75cm).Follow-up angiography showed improved flow in the main portal vein, and the stent was confirmed to be patent. Additionally, there were no procedure-related complications. Subsequently, while performing tract embolization, three 4mm x 10cm interlock coils and a mixture of 1:2 glue/lipiodol (2 vials of NBCA) were utilized, and the sheath was removed.
The patient was discharged after the procedure and is scheduled for outpatient follow-up in two weeks.
Portal vein stent patency will be checked through CT.