Paitent history)
A 52 year-old female patient presented E.R with dysarthria and general weakness started from 1 weeks ago.
The patient had history of head trauma 2 weeks before the presentation and hospitalized for 3days
He was told that the electrolyte lab was not normal in the first hospital but didn’t know the exact number.
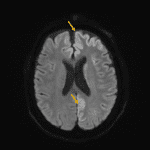
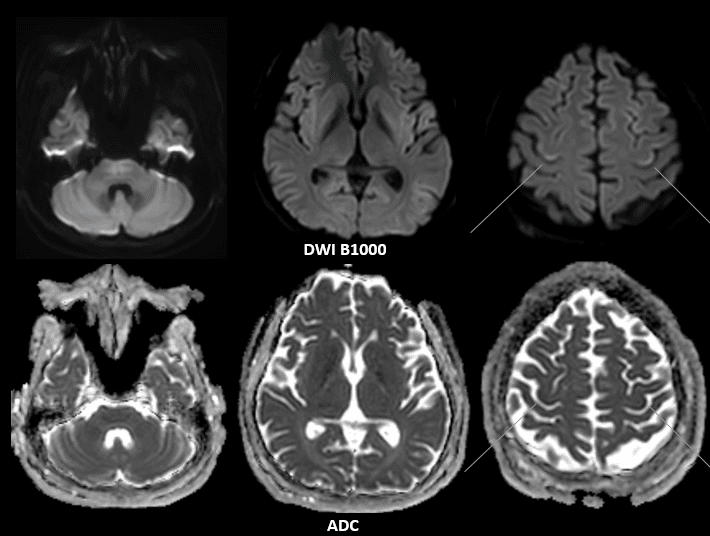
Let’s see the inital MRI



Laboratory finding of the patient
- Na(S), EM 137
- K(S), EM 3.8
- Cl(S), EM 102
- TCO2(S), EM 20
- Osmolality(S), EM 283
Osmotic demyelination syndrome
- Osmotic demyelination syndrome is acute demyelination caused by rapid shifts in serum osmolality
- Classic setting
- Rapid correction of hyponatremia (>10 mmol/L/day)
- Renal failure patients on dialysis, liver failure, malignancies such as lymphoma, carcinoma, cachexia, sepsis, acute pancreatitis, and chronic alcoholism
- Manifestation
- Quadriparesis and pseudobulbar palsy (involvement of corticospinal and corticobulbar tracts in pons)
- Extrapyramidal symptoms, such as rigidity, myoclonus, movement disorders, and parkinsonism-like features (EPM)
- Central pontine myelinolysis (CPM)
- Noninflammatory demyelination centered within the pons
- Peripheral fibers spared
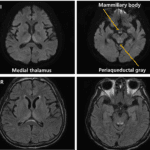
- Extrapontine myelinolysis (EPM)
- Commonly occurs in conjunction with CPM (but, also may be seen in isolation.)
- Common site – basal ganglia, thalamus, and cerebral white matter
- Less common site – peripheral cortex, hippocampi, and lateral geniculate bodies
- CPM + EPM = almost pathognomonic for ODS
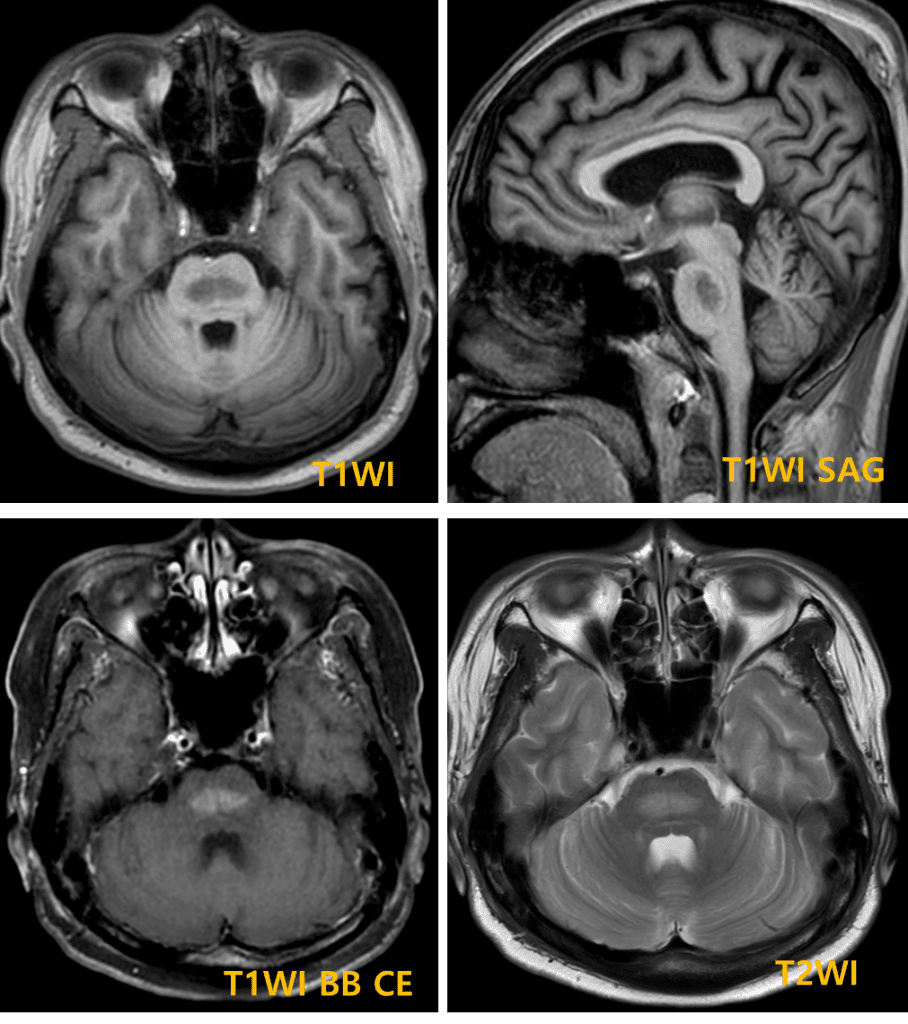
- MR Findings
- T1WI
- Acute : mildly/moderately hypointense, can be isointense with surrounding normal brain
- Subacute : may resolve completely, hyperintensity at 1-4 months (coagulative necrosis)
- T1WI C+
- Usually not enhance, less commonnly confluent/peripheral enhancement
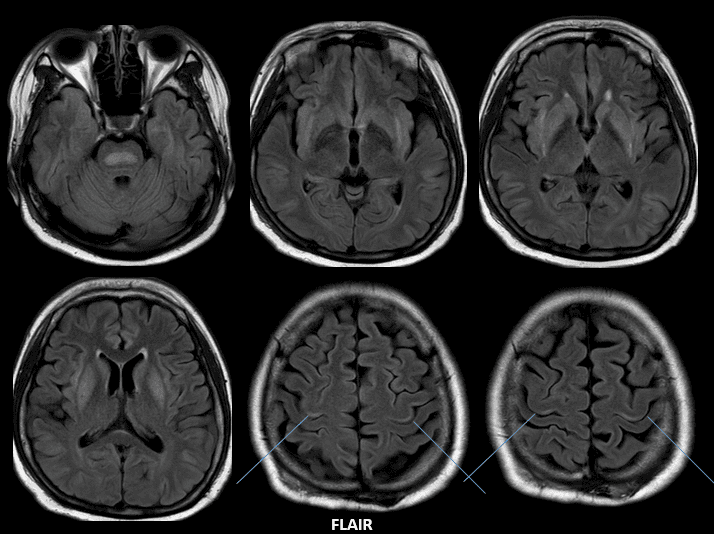
- T2WI/ T2 FLAIR
- Acute: Confluent hyperintensity in central pons with sparing of periphery and corticospinal tracts
- Subacute: normalizes and may resolve completely
- DWI
- Acute: Hyperintense (restricted) with ADC hypointense value
- Delayed: normalization within within 3-4 weeks
- DWI earliest and sensitive for ODS
- DWI changes occur within 24 hours of symptoms
- T1WI
References)
Turner MR, et al.Pract Neurol 2017;0:1–2. doi:10.1136/practneurol-2017-001682
RadioGraphics 2009; 29:933–938 • Published online 10.1148/rg.293085151 J Neuroimaging 2018;28:139-149. DOI: 10.1111/jon.12493