Hair wire fracture during insertion of PCD


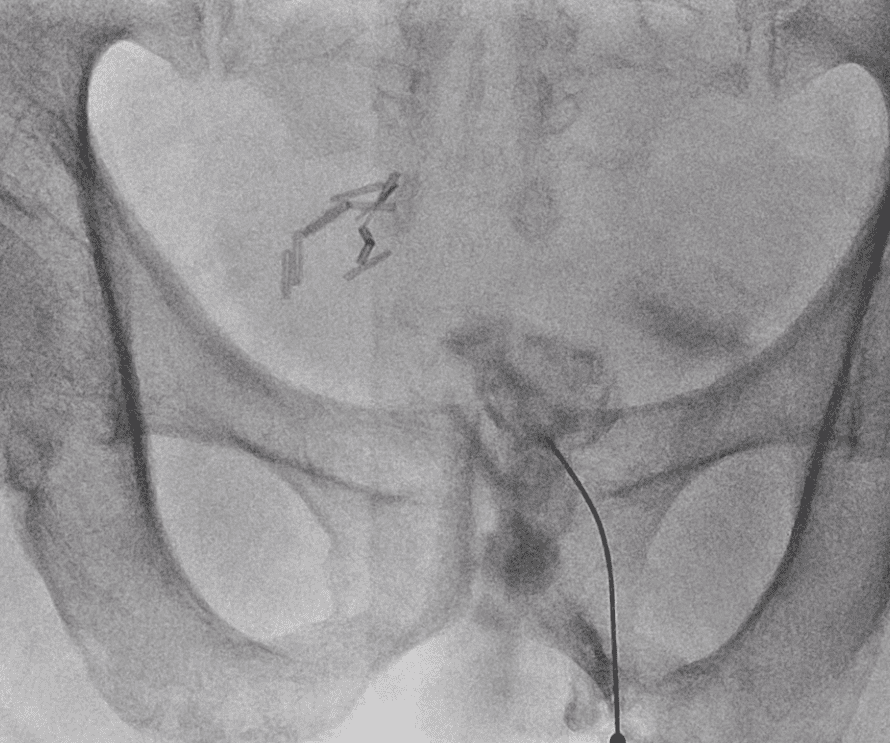



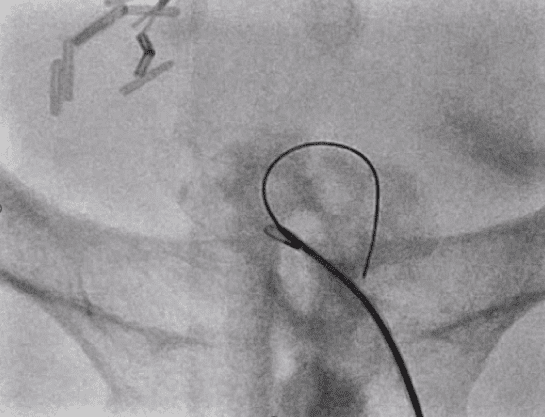


As a result, a new puncture was performed, and a PCD tube was inserted.
The fractured guidewire was planned to be removed at a later time.


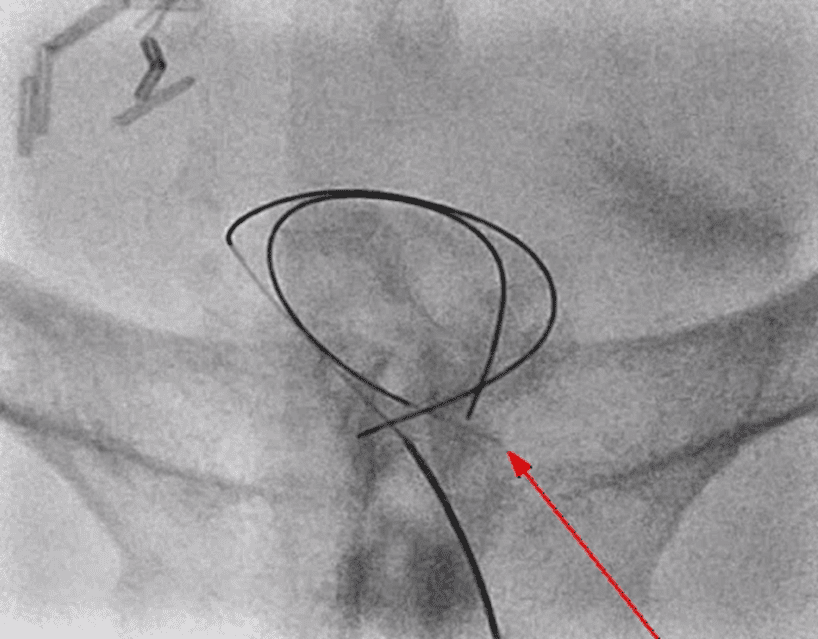
Through the existing PCD tract, we attempted to insert an 8Fr sheath and maintained the tract with a 0.035″ guidewire. We made multiple attempts at hair wire removal using a 20mm snare and biopsy forceps but were unsuccessful. We plan to try again the next day using a different type of snare.


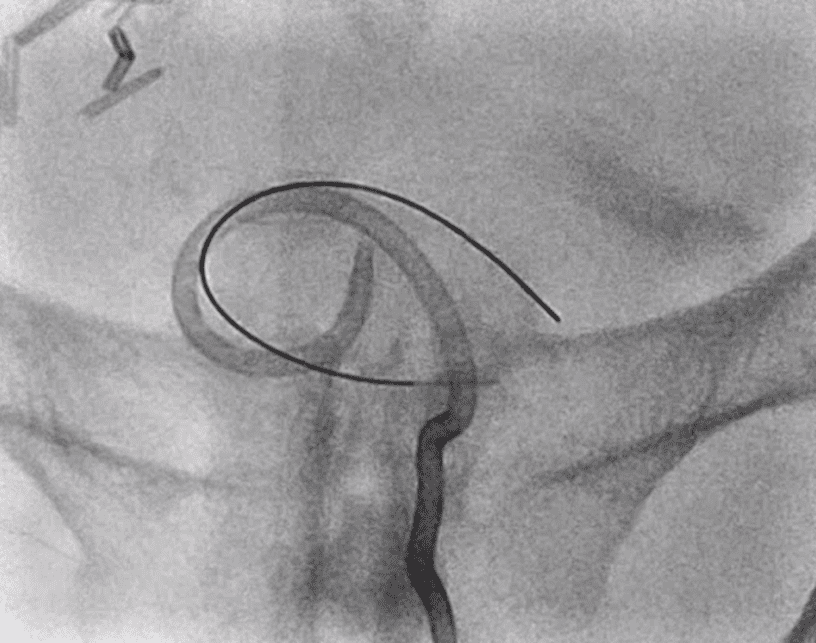
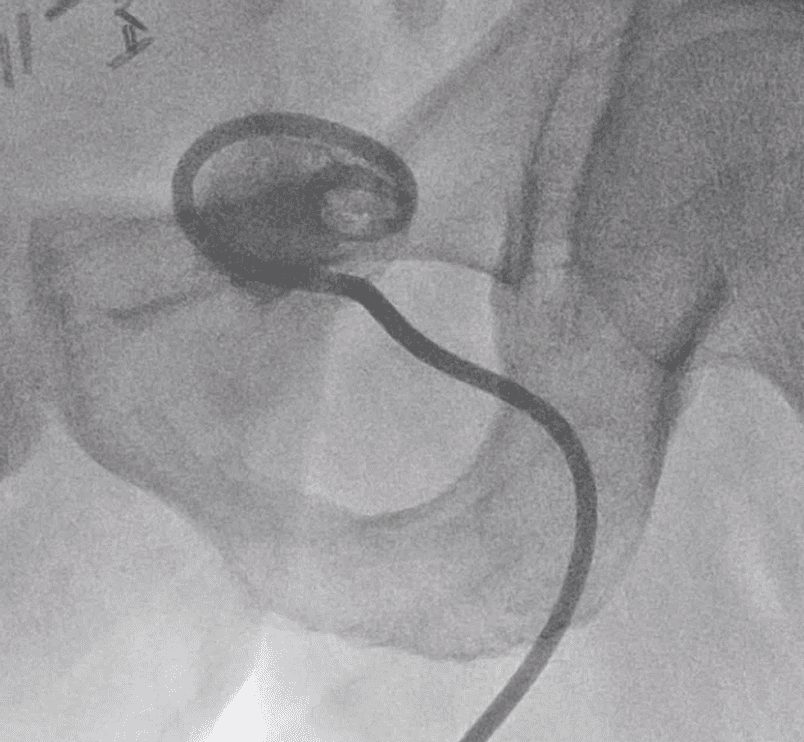
Through the existing PCD tract, we inserted an 8Fr sheath. We inserted a 0.035″ guidewire to maintain the tract while making multiple attempts to capture the broken hairwire using a snare. We successfully captured and retrieved the hairwire; however, the hard tip was embedded in the surrounding tissue, allowing us to withdraw it only as far as the sheath interior. After confirming that the floppy tip was almost reaching the skin, we used a mosquito clamp under fluoroscopy guidance to grasp and remove the tip.

Today, we discussed the case of potential 0.018″ guide wire fracture during PCD tube insertion and the subsequent removal of the fractured guide wire.
I searched the literature for similar cases and found one where a wire had entered a liver abscess cavity and was removed using biopsy forceps. However, I couldn’t find conclusive evidence regarding the impact of leaving a guide wire in the cavity’s tissue or whether it must be removed. Nevertheless, We decided to remove it, as the presence of a foreign body in an inflamed space could potentially contribute to the continuation of inflammation.


